Download
1 / 22
240 likes | 521 Views
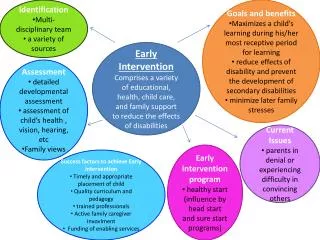
Why early identification of HL ?. Early intervention is possible only after early identification Early intervention allows more effective habilitation of HL. Methods of early identification. Screening High level of suscpicion Continuous education of health care professionals

E N D
Why early identification of HL ? Early intervention is possible only after early identification Early intervention allows more effective habilitation of HL
Methods of early identification • Screening • High level of suscpicion • Continuous education of health care professionals • Increasing public awareness
Screening • Specific medical intervention • Aim: Detection of disease or disability earlier that without screening • More effective intervention after screening than without screening
Screening • Population: • Screening: primarily healthy population • Diagnostic: disease suspected • Ratio of benefit to risks must be judged differently • Usually no quantifying results
Screening screening test + “fail” “pass” inefficient screening disease present disease not present disease present disease not present
Screening assessment of hearing (Audiometry) • Methods: • subjective • objective • Clinical use: • screening • diagnosis • quantification
Screening Test: OAE or AEP + “fail” “pass” inefficient screening disease present disease not present disease present disease not present
TEOAE „always“ present TEOAE „always“ missing
TEOAE + TEOAE missing
Number of ears with severe SNHL n=36 Passcriteria: SNR 5 dB; [in parenthesis 7dB] Pass rates in a test cavity “DPOAE” measurements (n=96); L1 = 65 / L2 = 55 dB SPL
CEOAEs stimulus level 90dB SPL peak CEOAEs stimulus level 83dB SPL peak
OAE Screening OAE present! no OAE no OAE no OAE
Use of OAE: Screening • Global screening of peripheral hearing function • No screening of neural function • Newborn hearing screening
screening for HL neonates + “fail” “pass” inefficient screening disease present disease not present disease present disease not present “true pos.” “false pos.” “false neg.” “true neg.” 1-3/1000 1-3% ? 97-99%
2. - 4. day Aim: covering all birth Organization and supervision: pediatricians Measurements: nurses, midwifes Follow up: pedaudiological services of otology departments Neonatal hearing screening inSwitzerland
Neonatal hearing screening inSwitzerland • TEOAEs on day 2 - 4 : 1 ear pass = screening passed • Fail on both sides: TEOAEs repeated before discharge • Second fail: pedaudiological examination 4 weeks later (appointment at discharge) • Pedaudiological examination: OAE measurements, if failed again ⇨ AEP in natural sleep
Neonatal hearing screening inSwitzerland Veraguth, Pieren, Schmid, Vischer, 2004 132 obstetric departments 3/4 with neonatal hearing screening
Neonatal hearing screening inSwitzerland Veraguth, Pieren, Schmid, Vischer, 2004 Births per year and NNH-screening
Neonatal hearing screening inSwitzerland Veraguth, Pieren, Schmid, Vischer, 2004 1999-2003: 50‘000 births 98.5 % pass, 1.5 % fail
Neonatal hearing screening inSwitzerland Veraguth, Pieren, Schmid, Vischer, 2004 Follow up of 751 fails 1 in 1000 baby with HL identified
Diagnosis of HL • Type of hearing loss: • Conductive • Sensorineural: cochlear? • Etiology of HL • Degree of HL (audiometry) • Degree of disability • other handicaps • Psychosocial background