Download
1 / 62
620 likes | 633 Views
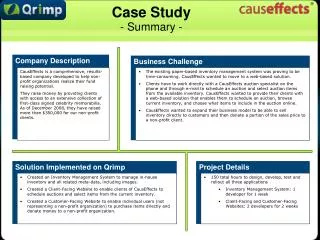
Explore the history, principles, and current challenges of the Canadian health care system. Learn about Medicare, public administration, and the role of provincial and federal governments in delivering health services. Understand the evolution from private medicine to universal health insurance. Examine key providers and ongoing issues like overcrowding, doctor shortages, and long waiting times.

E N D
About the case summary • 12 Font size Times New Roman • Average 2-3 pages • Name and student number • First case summary due on September 26
Canadian health care systems: the past and the future Objectives: • Understand principles of Canadian health care system • Understand its evolution and how the system works • Understand the current problems in the system
QuizTesting your knowledge about the Canadian Health Care System • The health insurance plan of a province must be administrated and operated on a non-profit basis by a public authority accountable to the provincial government. True False
Medically services provided by hospitals and physicians are covered by Medicare. True False
All people living in Canada are entitled for the insured health services on uniform terms and conditions. True False
Additional charges to insured patients for insured services are not allowed. True False
Canadian residents are entitled to coverage when they move to another province within Canada, but not covered when they travel aboard. True False
Principles of Medicare • Public administration • Comprehensiveness • Universality • Accessibility • portability
Canadian health care system • Publicly financed, privately delivered The responsibility of provincial government - Management and delivery of health care services The responsibility of federal government – Setting and administering of national principles or standards for the health care system assisting in the financing of provincial health care services through fiscal transfers, fulfilling functions for which it is constitutionally Responsible, and responsible for health protection, disease prevention, and health promotion.
Rely extensively on primary care physicians • Account for 51% of all active physicians in Canada • Paid on fee-for-services basis • Act as “gatekeeper” of the Canadian health care system
95% hospitals are non-profit entities • Run by community boards of trustees, voluntary organizations or municipalities. • Accountable to the communities they serve, not to the provincial bureaucracy
Evolution of universal health insurance • Prior to 1940’s, private medicine dominated health care in Canada resulting in access to care being based on ability to pay.
Evolution (contd.) • 1947 the province of Saskatchewan introduced a public insurance plan for hospital services • 1956 federal government, seeking to encourage the development of hospital insurance programs in all provinces, offered to cost-share hospital and diagnostic services on a roughly fifty-fifty basis.
Evolution (contd.) • By 1961, all ten provinces and the two territories had signed agreements establishing public insurance plans that provided universal coverage for at least in-patient hospital care that qualified for federal cost-sharing.
Evolution (contd.) • Public medical care insurance began in the province of Saskatchewan, providing coverage for services provided by physicians outside hospitals. • By 1972, all of the provincial and territorial plans had been extended to include physicians’ services. The objective to have a national health insurance plan for hospital and medical care in Canada had been realized.
How does the system work? • Payers • Provincial government – Ministry of Health (MOH) • Covers insured hospital and physician services • Covers costs of certain non-insured services for certain specific population groups • Controls the rate of adopting and diffusing expensive medical technology
Insurance companies • Cover a range of health services that remain outside the national health insurance framework • Workplace safety and insurance board • Provide insured benefits to workers with work-related injuries or illness
Providers • Hospitals: teaching hospitals, general/community hospitals, small hospitals and mental health hospitals • Physicians: general physicians and specialists • nurses
Other health care providers • Include dentists, chiropractors, opticians, occupational therapists, etc. • Voluntary organizations • Ontario Gerontology Association (is an incorporated voluntary organization concerned with aging, thereby promoting quality of life for older adults. Its membership provides an inter-disciplinary forum for those involved in the field of gerontology)
Problems in the health care system • Emergency overcrowding • Doctor shortage • One in four Ontario doctors will retire in four years • By 2020, 30% of Ontario’s population will be over the age of 55. • Waiting time • Access to health care providers, diagnostic tests, specialty treatment, hospital beds
Waiting time examples: • Six months to obtain a hip replacement • Five months to get a CAT scan • Some patients wait more than a year for cardiac surgery • Some cancer patients go to the States for treatment • 2/3 Canadian physicians are finding it difficult to get appropriate resources such as diagnostic tests, referrals or operating room time for their patients.
Waiting time for the access to health care services • Waiting time for unmet need and/or inadequate resources within the health care system
Environmental factors • Aging population (30% of Ontario population over 55) • Physicians leave outnumber those who have returned • ¾ family physicians are unable to accept new patients • Funding constraints • People demands high quality services
Long-term impact • Personal life • Work • Economic development • The Canadian health care system is one of the central determinants of our industrial competitiveness and our quality of life. (Conference Board of Canada, 1998)
Causes • The system • Organized around acute care, rather than chronic care (reactive vs. proactive) • Task-oriented rather than customer-oriented • Lack of integration • Lack of cost-saving incentives • Hospitals • Physicians • patients • Gatekeeper, is it necessary?
Ourselves • Lack of medical knowledge • Misuse • Healthy life style
Changing paradigm Old New acute care continuum of care treating illness maintaining and promoting wellness Individual patients defined population Provider similar differentiation Inpatient admission people health Fill beds provide timely care Separate org. Integrated system Run organization oversee a market Managers as depart.heads operate across organizations Coordinate services purse quality improvement
Reforming the Canadian health care system • Reforming primary health services (150 physicians, 220,000 patients, 7 sites) • Availability of a nurse practitioner to enhance access to primary care • 24-hour access to care • No change in the waiting time • Quality of care is considered to be good or very good • Patients were very satisfied
Hospital Services Restructuring Committee (HSRC) • Horizontal integration within the hospital sector • Result in extensive cost reduction and rationalization of services within the hospital sector • But heavier load for hospital personnel
Physicians • High level of satisfaction except those in Chatman • No change in their practice patterns • Some found unable to offset the extra costs of information technology • Found difficult in providing on-all coverage (since they can’t bill for the telephone advice) • Unrealistic expectations from the government • Information technology acquisition process (lengthy, resource-intensive, inefficient, and fragmented)