Download
1 / 10
100 likes | 139 Views
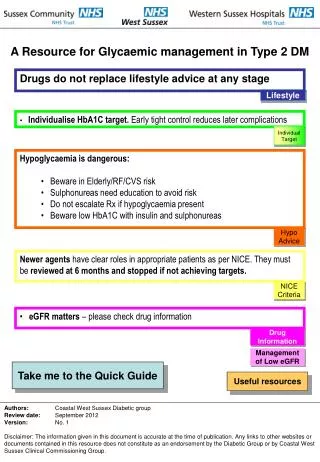
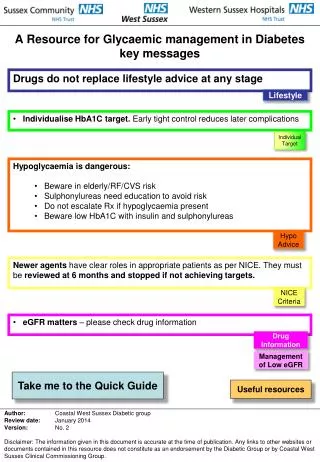
This resource provides key messages for managing diabetes, emphasizing lifestyle over drugs and individualized HbA1C targets. It covers hypoglycaemia risks, newer agent roles, and drug management based on eGFR. Useful resources and advice on insulin, sulphonylurea pathway, and lifestyle interventions are included.

E N D
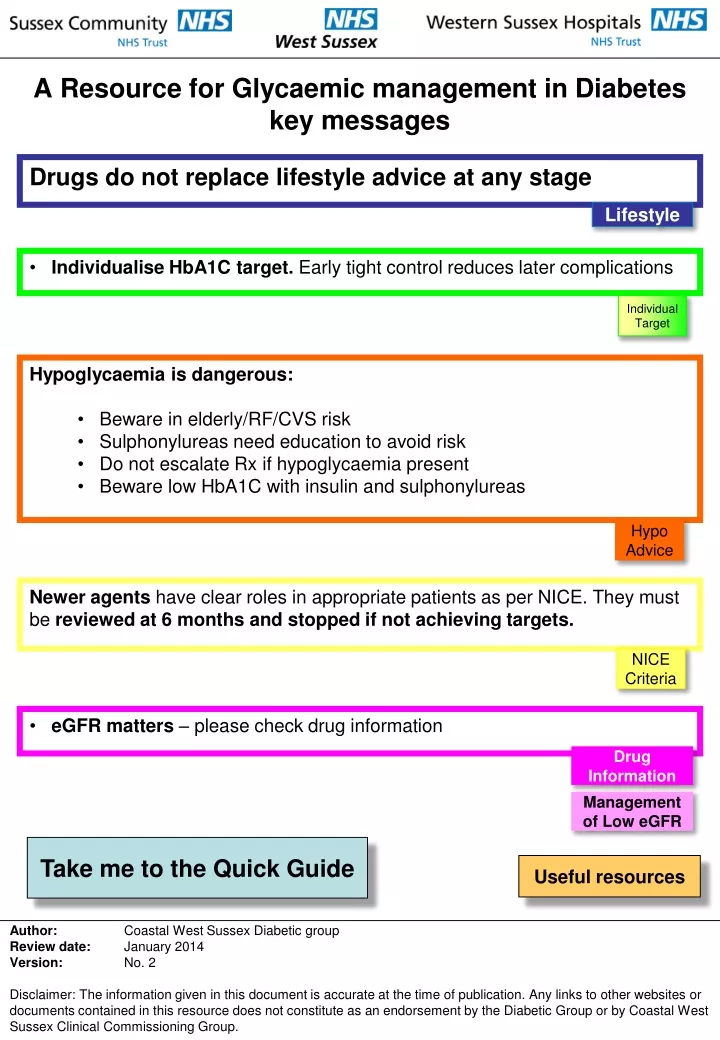
A Resource for Glycaemic management in Diabeteskey messages Drugs do not replace lifestyle advice at any stage Lifestyle • Individualise HbA1Ctarget. Early tight control reduces later complications Individual Target • Hypoglycaemia is dangerous: • Beware in elderly/RF/CVS risk • Sulphonylureas need education to avoid risk • Do not escalate Rx if hypoglycaemia present • Beware low HbA1C with insulin and sulphonylureas Hypo Advice Neweragents have clear roles in appropriate patients as per NICE. They must be reviewed at 6 monthsandstopped if notachieving targets. NICE Criteria • eGFR matters – please check drug information Drug Information Management of Low eGFR Take me to the Quick Guide Useful resources Author: Coastal West Sussex Diabetic group Review date: January 2014 Version: No. 2 Disclaimer: The information given in this document is accurate at the time of publication. Any links to other websites or documents contained in this resource does not constitute as an endorsement by the Diabetic Group or by Coastal West Sussex Clinical Commissioning Group.
Quick Guide: Blood Glucose Lowering Therapy in Type 2 DM Diagnosis • Symptomatic of hyperglycaemia requiring rapid control / low BMI • Metformin contraindicated or not tolerated Diet and lifestyle tried HbA1C > 48 (6.5%) Consider Sulphonylurea pathway page 2 Individual Target Lifestyle Metformin At risk from hypoglycaemia or Gliclazide side effects not tolerated / unacceptable HbA1C > 48 (6.5%) or individualised target Lifestyle NICE Criteria Individual Target Metformin + Gliclazide (Repaglanide if lifestyle erratic) Metformin + Gliptin or Pioglitazone Drug Information Hypo Advice Management of Low eGFR HbA1C > 58 (7.5%) HbA1C > 58 (7.5%) Individual Target Individual Target Lifestyle Lifestyle High BMI? See NICE criteria for GLP1 agonist use- (refer DSN fprinitiation) Do not fit NICE criteria for GLP1 agonist or Insulin unacceptable Insulin acceptable? NICE Criteria Start Insulin Consider Metformin +/- Gliclazide + Exenatide or Liraglutide Hypo Advice Insulin Button Consider triple RX Metformin Gliclazide + Gliptin or Pioglitazone Hypo Advice Intensify Insulin +/- Metformin +/- Pioglitazone +/-Gliptin Monitor 6/12 Target Hypo Advice HbA1C> 58 (7.5) Target not met Useful resources Change to insulin Hypo Advice Insulin Button Start Insulin +/- Metformin +/- Pioglitazone +/- Gliptin Insulin Button Home Adapted from NICE Clinical Guideline 87, Type 2 Diabetes (May2009)
Sulphonylurea Pathway Poor initial response V low BMI Exclude underlying pathology May need insulin, (type1?) refer Gliclazide Hypo Advice Metformin tolerated Return to Metformin pathway (page1) Consider stopping Gliclazide if initial response rapid > HbA1C 52 (7%) or individualised target Lifestyle Individual Target Metformin not tolerated or contraindicated then consider Gliptinor Pioglitazone Gliclazide + Gliptinor Pioglitazone > HbA1C 58 (7.5%) or individualised target Individual Target Lifestyle Start Insulin Hypo Advice Intensify Insulin regimen Drug Information Home Useful resources Management of Low eGFR Take me back to the quick guide, page 1 Adapted from NICE Clinical Guideline 87, Type 2 Diabetes (May2009)
Lifestyle interventions Education – Type1 – needs a link Type2 -needs a link Care Planning with individualised Targe • Year of Care Link Diet • Who should see the Dietitian? • Diet sheets • Diet advice – Click hereto access the Eat well with DM2 DUK web page Weight – Needs updating • Weight loss Help – click hereto access the Why Weight page on the GP website • Why Weight: Tel 0300 123 0892 Exercise • Exercise Referral Smoking • Stop Smoking advice: Tel 0300 100 1823 Mood Matters – MMG/TTT/Psychology Self Help signposting – Wellbeing hub Contact numbers Home Take me back to the quick guide
Hypoglycaemia Advice • Hypoglycaemia IS DANGEROUS Always enquire about mild symptoms especially with HbA1C <7 Teach patients to actively pre-empt low blood sugar & know how to manage hypoglycaemia. • Emergency treatment of hypoglycaemia • Ongoing management / advice for hypoglycaemia • Patient leaflet – management advice on hypoglycaemia • Driving and hypoglycaemia advice • Medical standards of fitness to drive Home Take me back to the quick guide
Aim Hb1C 48-53mmol/mol (6.5-7%) Younger patient Newer diagnosis Low risk of hypoglycaemia No co-morbidities Micro-vascular complications AimHbA1C58mmol/mol (7.5% or higher) Older patient Long standing diabetes Multiple hypoglycaemic agents Cardiovascular risk Macro-vascular complication Individualised Target • When setting a target HBA1C): • Involve the person in decisions about their individual HbA1C target level, see above • Encourage the person to maintain their individual target unless the resulting side effects • (including hypoglycemia) or their efforts to achieve this impair their quality of life • Offer therapy (lifestyle and medication) to help achieve and maintain the HbA1C target level • Inform a person with a higher HbA1C that any reduction in HbA1C towards the agreed target is advantageous to future health • Avoid pursuing highly intensive management to levels of less than 48mmol/l or 6.5 %. • However in early disease tight control (HbA1C 48mmol/mol or 6.5%) holds better long-term outcome Home Take me back to the quick guide
Insulin • Insulin should be initiated by qualified practitioners only. Dietitian input should also be sought at the same time • Aims of treatment with insulin • Leaflets: • Sick day rules • Implication of Ketone levels • Simple dose adjustment instructions: • QDS / Basal Bolus • BD / pre-mix • Hypoglycaemia awareness (advice see hypoglycaemia page) • Link to safe use of insulin on NHS Diabetes website • Download the Insulin Passport Hypo Advice Home Take me back to the quick guide
NICE Criteria DPP-4 inhibitors (Sitagliptin, Vildagliptin, Saxagliptin, Linagliptin) • ContinueDPP-4 inhibitor therapy only if there is a reduction of ≥ 0.5 percentage points in HbA1c in 6 months. • Discuss the benefits and risks of a DPP-4 inhibitor with the person, bearing in mind that a DPP-4 inhibitor might be preferable to a Thiazolidinedione if: – further weight gain would cause significant problems, or – a Thiazolidinedione is contraindicated, or the person had a poor response to or did not tolerate a Thiazolidinedione in the past. GLP1 agonists (Exenatide/ Liraglutide) These shouldonly be initiated by the team with special interest in practice • Discuss the benefits of GLP1 agonist to allow the person to make an informed decision. Consider starting in: • BMI ≥ 35 kg/m2 in people of European descent and there are problems associated with high weight, or • BMI < 35 kg/m2 and insulin is unacceptable because of occupational implications or weight loss would benefit other co-morbidities. 6 month review • Continue GLP1 Therapy only if the person has a reduction in HbA1C of ≥ 1.0 percentage point and ≥ 3% of initial body weight in 6 months. Thiazolidinedione (Pioglitazone) • Continue Thiazolidinedione therapy only if there is a reduction of ≥ 0.5 percentage points in HbA1c in 6 months. • Discuss the benefits and risks of a Thiazolidinedione with the person, bearing in mind that a Thiazolidinedione might be preferable to a DPP-4 inhibitor if: – the person has marked insulin insensitivity, or – a DPP-4 inhibitor is contraindicated, or – the person had a poor response to or did not tolerate a DPP-4 inhibitor in the past. • Do not start or continue a Thiazolidinedione if any suspicion or risk of bladder cancer/ frank haematuriaif the person has heart failure or is at higher risk of fracture. • When selecting a Thiazolidinedione, take into account the most up-to-date advice from regulatory authorities, cost, safety and prescribing issue Click here to access the full NICE guidance Home Take me back to the quick guide Adapted from NICE Clinical Guideline 87, Type 2 Diabetes (May2009)
Management of Low eGFR Prescribers should always check the latest product information in the relevant data sheet by visiting http://www.medicines.org.uk/emc/ Home Take me back to the quick guide
Useful Resources Diagnostic criteria • WHO. • Quick summary chart Referral protocols • Dietitian • DSN • Footcare clinic Information Leaflets For the patient: • Diet sheets • Driving and the new medical standards for people with diabetes • Footcare instructions • Hypoglycaemia dietary advice For the Clinician • Mood Management Referral – needs link • Preconception Consultation • Emergency Hypoglycaemia Treatment • Guidelines for Blood Glucose Meter testing use – Type1 Type2 Useful Websites • HBA1C conversion chart • Link to safe use of insulin on NHS Diabetes website • Click here to access the DVLA Guide to Medical Standards of fitness to drive • Click here to access the Map of Medicine • Click here to access the NICE pathway for a Diabetes overview • Click here to access Diabetes UK • Click here to access DUK – Understanding Diabetes • Click here to access Diabetes Bible Contact Details • Hospital contact details • Worthing Diabetes Centre 01903 285044 (9am – 4pm, Mon - Fri) • St Richards Diabetes Centre 01243 831614 (9am - 4pm, Mon - Fri) • Email Sc-tr.communitydiabetesservice@nhs.net Home Take me back to the quick guide