Download

1 / 17
180 likes | 369 Views
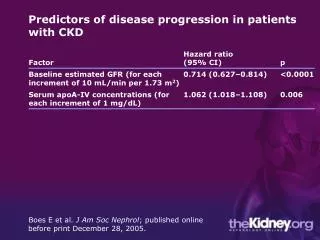
ESAs and Outcomes in CKD Patients. Philip Lui PharmD The 13th Annual Contemporary Therapeutic Issues in Cardiovascular Disease May 8, 2010. Anemia in CKD Patients.

E N D
ESAs and Outcomes in CKD Patients Philip Lui PharmD The 13th Annual Contemporary Therapeutic Issues in Cardiovascular Disease May 8, 2010
Anemia in CKD Patients • Associated with impairment in quality of life, reduced energy, neurocognitive decline, decreased exercise capacity, and increased mortality • Erythropoiesis-stimulating agents (ESAs): epoetin alfa, epoetin beta, darbepoetin alfa
Hemoglobin Targets Significantly higher primary end point of death, MI, hospitalization for CHF, or stroke in higher hemoglobin target group No significant difference NEJM 2006;355:2071-84, NEJM 2006;355:2085-98
Normal Hematocrit study NEJM 1998;339:584-90
TREAT • Randomized, double-blind, placebo-controlled trial • 4038 patients with type 2 diabetes, chronic kidney disease not on dialysis and anemia • Darbepoetin to increase Hb to 130g/L versus placebo with rescue darbepoetin if Hb < 90g/L
TREAT NEJM 2009;361:2019-32
TREAT Darbepoetin group • More thromboembolism (2.0% vs. 1.1%) • More deaths from cancer among patients with history of cancer (7.4% vs. 0.6%) • Fewer transfusions (14.8% vs. 24.5%) • Quality of life scores
Implications • Placebo controlled • Largest trial with the most adjudicated events • Did not confirm the higher rates of death and hospitalization for CHF in CHOIR • Darbepoetin confers no benefit in mortality or cardiovascular or renal outcomes compared to placebo
Stroke Risks CHOIR, CREATE • No difference Normal Hematocrit study • High Hct 6.3% vs. low Hct 4.7% (p=ns) Canadian-European Normalization of Hemoglobin with Erythropoietin trial • High Hb 4% vs. low Hb 1% (p<0.05) NEJM 1998;339:584-90, J Am Soc Neph 2005;16:2180-9
Potential Mechanisms • Increased viscosity and wall shear stress • Thrombocytosis • Increased platelet reactivity, adhesion, and aggregation • Increased arterial pressure Am J Kidney Dis 2009;53(5):733-6, Adv Chronic Kidney Dis 2009;16(2):131-42
TREAT Quality of Life • FACT–Fatigue • Improvement in mean score - darbepoetin 4.2 vs. placebo 2.8 • Clinically meaningful change of 3 points - darbepoetin 55% vs. placebo 50% • SF-36 • No significant difference
Quality of Life CHOIR (LASA, KDQ, SF-36) • Both groups improved, no significant difference CREATE (SF-36) • Significant improvements in high Hb target group
Outstanding Unknowns • Dose • Hemoglobin target • ESA hyporesponsiveness • Different dosing strategy • Class effect • Patient population • Quality of Life
Treatment of Anemia CKD patients not on dialysis • Minimize ESA use for mild to moderate anemia (90-110g/L) especially for those with minimal fatigue • Minimize ESA use for those with history of cancer or stroke • Transplant candidates or those with severe anemia (<90g/L) may consider long term ESA to maintain Hb between 90g/L and 110g/L J Am Soc Neph 2010;21:1-13
Treatment of Anemia Dialysis patients • Use lowest dose to maintain Hb above 90g/L • Pursue other strategies to lower ESA dose (eg. SC instead of IV, peritoneal dialysis, iron, treat inflammation) • Minimize ESA use in patients who are within 2 years of diagnosis of malignancy J Am Soc Neph 2010;21:543-55