Download
1 / 13
130 likes | 142 Views
This study explores the significant role of a public health registrar in tackling tuberculosis in the West Midlands, highlighting the region's challenges and progress in TB control. The registrar's perspective sheds light on coordinating actions with various partners to address this critical public health issue. Case studies include contact tracing in high TB incidence areas, designing latent TB testing pathways for asylum-seeking children, and reviewing neonatal BCG vaccine policies. Key learning opportunities emphasize collaboration, understanding challenges, and achieving long-term impact in TB control. Acknowledgements to public health experts who contributed to this research.

E N D
Tackling TuberculosisThe contribution of a public health registrar in different settings within the West Midlands Helen Green Public Health Registrar (ST3) West Midlands
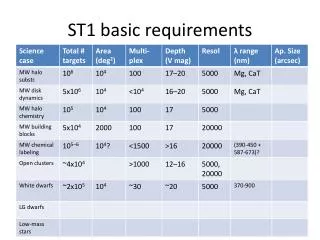
Tuberculosis in the West Midlands • 2. Highest regional rate in non UK born in England • 3. Highest regional proportion with multiple social risk factors in England • 1. Second highest regional rate of TB behind London • 4. Significant reduction during the past few years • 5. Considerable variation within the region PHE 2016 Tuberculosis annual report (presenting data to end of 2015)
How to tackle TB Tackling TB requires the coordinated action of many partners
A registrar’s perspective Unique opportunity to experience the perspective of different organisations and how they can contribute to addressing this public health issue Registrar
Local incidents requiring contact tracing in high TB incidence areas • An infectious case of TB working in a large factory for several months • Risk assessment carried out • Infectiousness, duration of contact, population vulnerability • Workplace contacts identified • A considerable number with different employment and shift patterns • High background prevalence of latent TB in workforce • Extension of screening required? • National PHE expert guidance • Whole Genome Sequencing
Designing a pathway for latent TB testing for unaccompanied asylum seeking children • UASC at an increased risk of TB infection • Responsibility of care lies with assigned local authority • Coventry and Warwickshire situation • Informal arrangements in place for the management of latent TB screening in this vulnerable group • Overlap between areas accepting UASC and areas placed • Variation in who carries out screening according to which GP registered with
Designing a pathway for latent TB testing for unaccompanied asylum seeking children (2) • A range of health and social care professionals consulted • Complex exercise to reconcile processes across Coventry and Warwickshire
Reviewing neonatal BCG vaccine policies in place across the West Midlands • BCG immunisation programme is risk-based • Neonatal programme a key component • Targeted at protecting children most at risk of exposure • Responsibility of Trust of birth • Selective strategy in the West Midlands • Requires identification of eligible neonates Clear pathways need to be in place • Restricted supply in 2015 and a change in vaccine highlighted variation in policy and practice by Trust in the region
Reviewing neonatal BCG vaccine policies in place across the West Midlands (2) • When identified? Training Data collection • Documentation? • Where vaccinated?
Implementing neonatal BCG vaccine policies in low incidence areas • Need to ensure standard recommended pathways appropriate to level of demand • Facilitates maximum uptake • Minimise vaccine wastage • Confirm contract arrangements between Trusts where necessary • Minimise impact of DNAs • Use of data available on the number of eligible neonates helps to engage the Trusts
Registrar benefits of experience in a range of settings Working in different settings afforded the opportunity to: 1. Explore different aspects of TB control, focusing on the following TB Strategy key areas: 2. Address the issue at different levels and through a range of perspectives 3. Observe the challenges faced when implementing best practice and when the level of need can vary markedly
Key learning opportunities Focusing on a common aim across training placements helps to: • Strengthen understanding of how organisations can work together to address key public health issues • Enable long term follow up of implementation of the work done and how it can result in change which can be difficult in time-limited placements TB incident management UASC pathway development BCG policy implementation BCG policy review June 2017 August 2016 August 2015
Acknowledgements • Nicola Benge (Consultant Lead Screening and Immunisation, PHE/NHS England West Midlands) • Nicky Bennett (Screening and Immunisation Coordinator, PHE) • Nadia Inglis (Consultant in Public Health, Warwickshire County Council and Coventry City Council) • Bharat Sibal (Lead CCDC, WME Health Protection Team, PHE) • Annette Wood (formerly Consultant Screening and Immunisation Lead, PHE/NHS England West Midlands)