Download
1 / 38
450 likes | 505 Views
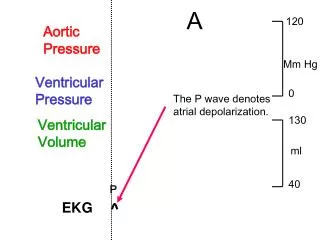
EKG Lecture. Scott Ewing, D.O. April 5, 2005. What is the rhythm in this 66-year-old woman?. Atrial Fibrillation. Atrial fibrillation with a rapid ventricular response (about 150 bpm) Non-specific ST-T changes are also noted. What arrhythmias are present in this middle-aged male?.

E N D
EKG Lecture Scott Ewing, D.O. April 5, 2005
Atrial Fibrillation • Atrial fibrillation with a rapid ventricular response (about 150 bpm) • Non-specific ST-T changes are also noted
Atrial Fibrillation • Atrial fibrillation (moderate ventricular response) and frequent premature ventricular complexes (PVCs) • The PVCs are multifocal with two distinct morphologies • The EKG does not show other specific abnormalities (the isolated Q wave in lead III is non-diagnostic)
Question • What arrhythmia is present in this wide-QRS-complex tachycardia? • Monomorphic ventricular tachycardia • Polymorphic ventricular tachycardia • Atrial fibrillation with left bundle branch block • Atrial flutter with left bundle branch block • Atrial fibrillation with Wolff-Parkinson-White pre-excitation
Atrial fibrillation with left bundle branch block • Note: The coarse atrial fibrillatory waves (lead V1) may be mistaken for atrial flutter waves • However, with fibrillation (verus flutter) the atrial activity varies continuously and usually the ventricular response is completely variable • QRS complex shows a typical LBBB morphology with secondary ST-T abnormalities
Question • What is the arrhythmia in this 73-year-old with very severe coronary disease, status-post inferior and anterior-lateral Q-wave myocardial infarction? • Atrial fibrillation • Atrial flutter with variable block • Multifocal atrial tachycardia • Sinus tachycardia with atrial premature beats • Atrial tachycardia with type I (AV Wenckebach) block
Atrial fibrillation • The highly irregular ventricular response and the variable, oscillatory atrial activity (see V1, e.g.) are classic for atrial fibrillation
Question • What arrhythmia is present in this elderly woman with a history of mitral valve replacement for rheumatic mitral valve disease? • Atrial flutter • Atrial fibrillation • Junctional rhythm • Sinus rhythm with frequent premature atrial complexes • Multifocal atrial tachycardia
Atrial Fibrillation • The patient had long standing atrial fibrillation • There are no discrete P waves which excludes sinus rhythm or multifocal atrial tachycardia • The erratic irregular oscillatory baseline with an erratic ventricular response is typical of atrial fibrillation • No flutter waves are seen
Bonus • What drug was she treated with?
Bonus • The scooping of the ST-T waves in the inferolateral leads are consistent with digitalis effect
Question • The following EKG shows which of the following? • Atrial flutter with 2:1 block • Atrial flutter with 3:1 block • Atrial flutter with variable conduction • Atrial fibrillation • Parkinsonian tremor artifact
Atrial Flutter with Variable Conduction • The EKG shows typical atrial flutter waves • The ventricular response is not highly irregular as in atrial fibrillation, but is also not strictly regular • The rate here has a definite pattern; the conduction is not constantly 3:1 or 4:1, but rather a combination of these intervals • Parkinsonian tremor may simulate atrial flutter or fibrillation • In such cases the underlying rhythm is usually recognizable upon close inspection.
Question • 55-year-old woman with rheumatic mitral valve disease and a narrow complex tachycardia. The rhythm is: • Sinus tachycardia • Atrial fibrillation • Atrial flutter with 2:1 AV conduction • AV nodal reentrant tachycardia • Ectopic atrial tachycardia
Atrial Flutter with 2:1 AV Conduction • Typical atrial flutter waves are present (negative in lead II; biphasic in V1) at a rate of about 270/min with 2:1 conduction • Note the non-conducted atrial flutter waves subtly present in the ST segment in V1 • Atrial flutter may mimic all of the arrhythmias given in the other choices • Relatively low voltage QRS complexes are also present in this patient who had pleural effusions
Question • What is the rhythm in this 79-year-old woman with complaint of shortness of breath? • Multifocal atrial tachycardia • Ventricular tachycardia • Atrial flutter/fibrillation with rapid ventricular response • Sinus tachycardia • Paroxysmal supraventricular tachycardia with AV nodal reentry
Atrial Fibrillation/Flutter with RVR • RVR rate of about 120 bpm with left axis deviation and a borderline intraventricular conduction delay • No evidence of discrete P waves, either normal or ectopic, excluding sinus tachycardia or a type of atrial tachycardia • Baseline shows some artifact with atrial flutter/coarse atrial fibrillatory activity • The regularized response at the beginning is consistent with flutter and the more erratic response response later suggests intermittent atrial fibrillation • Not uncommonly, these two "cousin" atrial tachyarrhythmias alternate or co-exist, so the term "fib-flutter" is used clinically
Question • 80 year-old man presented to emergency department complaining of fatigue and shortness of breath? What is the rhythm? • Sinus tachycardia • Atrial tachycardia • AV nodal reentrant tachycardia (AVNRT) • Atrial flutter with 2:1 conduction • Atrial fibrillation
Atrial Flutter with 2:1 Block • Atrial rate is 320 with 2:1 AV block (conduction), yielding a ventricular response is 160 bpm • Classic flutter “F” waves (consistent with a typical counterclockwise right atrial reentrant circuit) giving a “saw tooth” appearance to the atrial activity • Resting rate of 160 bpm excludes sinus tachycardia in this age group • Atrial fibrillation is ruled out because of the regularity of the ventricular response • Apparent flutter waves at 320/min exclude AVNRT or atrial tachycardia • Patient was treated with CCB for rate control and electrically cardioverted to sinus rhythm
Question • Tachycardia and a touch of cyanosis (rhythm and blues) • What is major finding in this patient with congestive heart failure (CHF)?
Atrial Flutter with Variable Conduction • Narrow complex tachycardia with atrial rate of about 300 indicating atrial flutter and slightly variable ventricular response (2:1 conduction, some 3:1 and probably some Wenckebach) • Atrial flutter is sometimes mistaken (by housestaff at other institutions) for sinus tachycardia • Look, for instance, at V1 where the flutter waves are hard to see vs. lead II where they are more apparent • If only a V1 type lead were available, the mechanism could be readliy mistaken
Question • Rapid palpitations. Why?
Atrial Flutter with 2:1 Conduction • Don't overlook subtle "extra" atrial wave (it's NOT a true P wave, but a flutter wave) in the early ST segment • Atrial flutter with 2:1 conduction is often mistaken for sinus tachycardia or paroxysmal supraventricular tachycardia (PSVT)
Bonus • 59-year-old female with sudden palpitations and lightheadedness
Atrial Fibrillation with WPW • Atrial fibrillation with the Wolff-Parkinson-White syndrome, with conduction down the bypass tract • (Mostly) wide complex tachycardia with a rate of about 230 beats/min • Differential diagnosis includes 1) ventricular tachycardia, 2) supraventricular tachycardia with aberrancy, and 3) WPW with conduction down the bypass tract • Major clues include the "irregularly irregular" rhythm and the extremely rapid rate • Ventricular tachycardia may be mildy irregular but this degree of irregularity would be unusual at this very fast rate • The short refractory period of certain bypass tracts can allow extremely rapid heart rates, especially during atrial fibrillation
Treatment • A correct diagnosis is very important because drugs that slow AV conduction (verapamil, beta blockers, digoxin, adenosine) are contraindicated • These drugs can facilitate preferential conduction down the bypass tract and the atrial fibrillation can degenerate to ventricular fibrillation • Drug of choice is IV procainamide and if this is unsuccessful, DC cardioversion should be performed promptly