Download

1 / 26
260 likes | 425 Views
Why Not the Best? Results from the National Scorecard on U.S. Health System Performance, 2011. Cathy Schoen, Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org October 18, 2011. 2011 Scorecard Methodology.

E N D
Why Not the Best? Results from the National Scorecardon U.S. Health System Performance, 2011 Cathy Schoen, Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org October 18, 2011
2011 Scorecard Methodology • Third edition: same framework and methods as previous editions • Five dimensions of health system performance: healthy lives, quality, access, efficiency, and equity • 42 indicators of health system performance • Scores are simple ratios of U.S. average to benchmark • Benchmarks are levels achieved by other countries or top U.S. states, regions, health plans, or providers (select indicators have policy goals or targets) • Updates benchmarks whenever they improved • To score dimensions, we average ratio scores for all indicators within dimension; dimension scores are then averaged for overall score • Time trends capture at least three years of data; more than two-thirds span 5+ years • Data primarily up through 2009, before reform
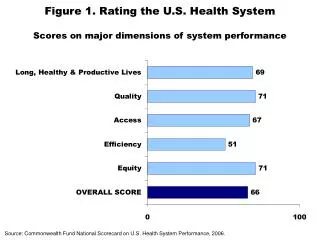
THE COMMONWEALTH FUND 2011 Scorecard Overview Findings: Overall Score is 64 out of 100 • Overall U.S. health system performance relative to benchmarks failed to improve between 2006 and 2011 scorecards • Performance compared with benchmarks improved on less than half of indicators • Wide disparities by income, race/ethnicity persist • Steep declines in access and affordability • Substantial variation across the U.S., with as much as fourfold spread • Uneven performance on quality, yet encouraging pockets of improvement • Rapid progress on quality metrics that have been focus of national initiatives and public reporting • Improvement on key quality metrics demonstrates significant progress possible when specific goals and targets set • Broad evidence of inefficient care and high costs • Substantial potential to improve
International Comparison of Spending on Health, 1980–2009 Total expenditures on healthas percent of GDP Average spending on healthper capita ($US PPP) *PPP= Purchasing power parity Source: OECD Health Data 2011 (June 2011). Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Scores: Dimensions of a High Performance Health System * Note: Includes indicator(s) not available in earlier years. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Mortality Amenable to Health Care Deaths per 100,000 population* * Countries’ age-standardized death rates before age 75; including ischemic heart disease, diabetes, stroke, and bacterial infections. See Appendix B for list of all conditions considered amenable to health care in the analysis. Data: E. Nolte, RAND Europe, and M. McKee, London School of Hygiene and Tropical Medicine, analysis of World Health Organization mortality files and CDC mortality data for U.S. (Nolte and McKee, 2011). Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Infant Mortality Rate Infant deaths per 1,000 live births U.S. National and State Trends International Comparison, 2007 ^ Denotes years in 2006 and 2008 National Scorecards. Data: National and state—National Vital Statistics System, Linked Birth and Infant Death Data (AHRQ 2003–2008; Mathews and MacDorman, 2011); international comparison—OECD Health Data 2011 (database), Version 06/2011. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Percent of Adults Ages 19–64 Uninsured by State 1999–2000 median = 15.0% 2009–2010 median = 19.4% 23% or more 19%–22.9% 14%–18.9% Less than 14% Data: U.S. Census Bureau, 2000–01 (revised) and 2010–11 Current Population Survey ASEC Supplement. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Steep Decline in Access: 81 Million Uninsured and Underinsured Adults, Up from 61 Million in 2003 Millions of adults ages 19–64 who are uninsured or underinsured, 2010 Percent of adults ages 19–64 who are uninsured or underinsured 44 42 35 52 102 29 Total: 184 million** * Underinsured defined as insured all year but experienced one of the following: medical expenses equaled 10% or more of income; medical expenses equaled 5% or more of income if low-income (<200% of poverty); or deductibles equaled 5% or more of income. ** Subgroups may not sum to total because of rounding. Data: 2003, 2007, and 2010 Commonwealth Fund Biennial Health Insurance Surveys. 9 Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Employer Premiums as Percentage of Median Household Income for Population Under Age 65 2003 2009 WA WA NH NH MT MT ME ND ME ND VT VT OR MN OR MN MA MA ID ID WI WI SD SD NY NY WY MI WY MI RI RI IA IA PA PA CT CT NE NE NJ NJ NV NV OH OH IN IN IL IL DE UT DE UT CO CA CO WV CA WV MD MD KS VA MO KS VA MO DC KY DC KY NC NC TN TN OK AZ OK AZ AR SC AR SC NM NM GA GA AL MS AL MS TX TX LA LA FL FL AK AK HI HI HI HI 18% or more 15%–17.9% 12%–14.9% Less than 12% Data: Average total premiums—2003, 2005, and 2009 Medical Expenditure Panel Survey; state median income for single and family households (all under age 65) —2003–2004, 2005–2006, and 2009-2010 Current Population Survey. 10 Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Medical Bill Problems or Medical Debt, 2010 Percent of adults ages 19–64 with any medical bill problem or outstanding debt* By income and insurance status, 2010 U.S. average * Problems paying or unable to pay medical bills, contacted by a collection agency for medical bills, had to change way of life to pay bills, or has medical debt being paid off over time. Data: 2005 and 2010 Commonwealth Fund Biennial Health Insurance Surveys. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Adults with an Accessible Primary Care Provider Percent of adults ages 19–64 with an accessible primary care provider* U.S. Average U.S. Variation 2008 * An accessible primary care provider is defined as a usual source of care who provides preventive care, care for new and ongoing health problems, referrals, and who is easy to get to and easy to contact by phone during regular office hours. Data: N. Tilipman, Columbia University analysis of Medical Expenditure Panel Survey. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Receipt of Recommended Screening and Preventive Care for Adults Percent of adults age 18+ who received all recommended screening and preventive care within a specific time frame given their age and sex* U.S. Average U.S. Variation 2008 * Recommended care includes at least six key screening and preventive services: blood pressure, cholesterol, Pap, mammogram,fecal occult blood test or sigmoidoscopy/colonoscopy, and flu shot. See Appendix B for complete description. Data: N. Tilipman, Columbia University analysis of Medical Expenditure Panel Survey. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. Chronic Disease Under Control: Diabetes and Hypertension U.S. Average By Insurance, 2005–2008 Percent of adults age 18+ Percent of nonelderly adults ages 18–64 *Refers to diabetic adults whose hemoglobin A1c is <9.0% **Refers to hypertensive adults whose blood pressure is <140/90 mmHg. Data: J. M. McWilliams, Harvard Medical School analysis of National Health and Nutrition Examination Survey.
Hospitals: Prevention of Surgical Complications Percent of adult surgical patients who received appropriate care to prevent complications* * See Appendix B for methods and description of clinical indicators. Data: IPRO analysis of data from CMS Hospital Compare. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Prescription of Potentially Unsafe Medications Among Elderly Beneficiaries, by Hospital Referral Regions, 2007 Percent of elderly Medicare beneficiaries Potentially harmful drug–disease interactions** Use of high-risk medication* * Medicare beneficiary received at least one drug from a list of 13 classes of high-risk prescriptions that should be avoided by the elderly. ** Medicare beneficiaries with dementia, hip or pelvic fracture, or chronic renal failure, and received a prescription in an ambulatory care setting that is contraindicated for the condition. Data: Y. Zhang analysis of 5% sample of Medicare beneficiaries enrolled in stand-alone Medicare Part D plans (Zhang et al., 2010). Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Medicare Hospital 30-Day Readmission Rates Remain High Percent of Medicare beneficiaries initially admitted for one of 45 medical conditions or surgical procedures who are readmitted within 30 days following discharge* U.S. average Hospital Referral Region percentiles, 2009 State percentiles, 2009 * See Appendix B for list of conditions and procedures used in the analysis. Data: G. Anderson and R. Herbert, Johns Hopkins University analysis of Medicare Standard Analytical Files (SAF) 5% Inpatient Data. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
18 Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011. Potentially Preventable Hospital Admissions for Select Ambulatory Care Sensitive Conditions Adjusted rate per 100,000 population* Heart failure Pediatric asthma Diabetes** * Rates are adjusted by age and gender using the total U.S. population for 2000 as the standard population. ** Combines three diabetes admission measures: uncontrolled diabetes without complications, diabetes with short-term complications, and diabetes with long-term complications. Data: U.S. average—Healthcare Cost and Utilization Project, Nationwide Inpatient Sample; State distribution—State Inpatient Databases; not all states participate in HCUP (AHRQ 2010).
Nursing Homes: Hospital Admission and Readmission Rates Among Nursing Home Residents, by Hospital Referral Regions Percent of long-stay nursing home residents hospitalized over a six-month period Percent of first-time nursing home residents rehospitalized within 30 days of hospital discharge to nursing home Data: V. Mor and Z. Feng, Brown University analysis of Medicare enrollment data and Part A claims data for all Medicare beneficiaries who entered a nursing home and had a Minimum Data Set assessment. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Use of Electronic Medical Records Percent of primary care physicians using electronic medical records United States International Comparison, 2009 AUS=Australia; CAN=Canada; FRA=France; GER=Germany; ITA=Italy; NETH=Netherlands; NZ=New Zealand; NOR=Norway; SWE=Sweden; UK=United Kingdom. Data: Commonwealth Fund International Health Policy Survey of Physicians. Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
International Comparison of Spending on Insurance Administration, 2009 a 2008 * Includes claims administration, underwriting, marketing, profits, and other administrative costs; based on premiums minus claims expenses for private insurance. NHE=National Health Expenditures Data: OECD Health Data 2011 (database), Version 06/2011. 21 Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Potential to Improve: National AnnualGains if Reach Benchmark Performance • Up to 91,000 fewer deaths before age 75 from causes potentially preventable with timely and appropriate health care if the U.S. achieved best country rate; 84,000 if achieved lowest 3 countries • 66 million more adults would receive recommended screenings and preventive care at appropriate ages according to guidelines • 38 million more adults ages 19–64 would have an accessible primary care provider • $55 billion in saving in insurance administrative costs if the U.S. achieved levels of other countries with competing private insurance plans • $114 billion if U.S. achieved levels of lowest rate countries • Does not include potential savings to physicians and hospitals from reduced complexity
Post-Reform: Projected Percent of Adults Ages 19–64 Uninsured by State 2009–2010 median = 19.4% 2019 (estimated) median = 8.4% WA WA NH NH MT MT ME ND ME ND VT VT OR MN OR MN MA MA ID ID WI WI SD SD NY NY WY MI WY MI RI RI IA IA PA PA CT CT NE NE NJ NJ NV NV OH OH IN IN IL IL DE UT DE UT CO CA CO WV CA WV MD MD KS VA MO KS VA MO DC KY DC KY NC NC TN TN OK AZ OK AZ AR SC AR SC NM NM GA GA AL MS AL MS TX TX LA LA FL FL AK AK HI HI 23% or more 8%–13.9% 19%–22.9% 14%–18.9% Less than 8% Data:U.S. Census Bureau, 2010–11 Current Population Survey ASEC Supplement; estimates for 2019 by Jonathan Gruber and Ian Perry of MIT using the Gruber Microsimulation Model for The Commonwealth Fund. 23 23 Source: Commonwealth Fund National Scorecard on U.S. Health System Performance, 2011.
Summary and Implications • Access is an essential foundation for improvement • U.S. losing ground in ensuring access to affordable health care • Access to care, health care quality, and efficiency are interrelated • What receives attention gets improved • Focused quality improvement and public reporting initiatives have led to significant gains • Measurable and actionable benchmarks provide targets to improve • Gaps between average performance and benchmarks remain large, underscoring potential gains • Better primary care and care coordination needed to improve outcomes at lower costs • Strengthen primary care system to ensure access, ongoing care management, and care coordination • Improve transitions and follow-up care after hospitalization needed • Align incentives to promote more effective and efficient use of staff, IT, and clinical resources
Affordable Care Act Reforms on Target • Insurance reforms will provide foundation for affordable, comprehensive insurance • Payment and care system reforms targeted on gaps, wide variations across the United States • Investment in information systems to guide and inform action • Emphasis on primary care and coordination, with patient-centered care teams • Accountability for health, care, and cost outcomes • Should expect to see positive scorecard results in the future
For More Information Visit the Fund’s website atwww.commonwealthfund.org Why Not the Best provides comparative data for hospitals. To access: www.whynotthebest.org