Download
1 / 15
150 likes | 531 Views
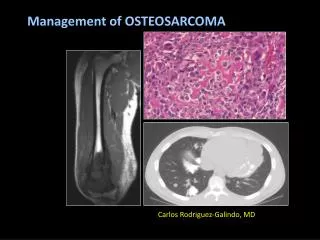
How Common are Bone Islands on Abdominal and Pelvic CT?. Tamar Sella MD Nurith Hiller MD Azraq Yusef MD Eugene Libson MD Jacob Sosna MD . Dept. of Radiology Hadassah Hebrew University Hospital, Jerusalem. Bone Islands - Background. focus of compact bone located in cancellous bone

E N D
How Common are Bone Islands on Abdominal and Pelvic CT? Tamar Sella MD Nurith Hiller MD Azraq Yusef MD Eugene Libson MD Jacob Sosna MD Dept. of Radiology Hadassah Hebrew University Hospital, Jerusalem
Bone Islands - Background • focus of compact bone located in cancellous bone • also known as an enostosis, endosteoma, calcified medullary defect • a benign entity that is usually found incidentally on imaging studies • bone islands may mimic a more agressive process, such as an osteoblastic metastasis
Bone Islands - Pathophysiology • exact etiology of bone islands is not clear • Most likely developmental in nature: cortical bone that has failed to undergo medullary resorption • Histologically, bone islands are intramedullary foci of normal compact bone with haversian canals and "thorny" radiations that merge with the trabeculae of surrounding bone • Hamartoma?
Bone Islands - Frequency • The exact frequency is unknown • Prevalence estimated as 0.6-1.4% based on plain radiographs • May be found in any osseous site; however, most commonly identified in the pelvis, long bones(most commonly proximal femur), also fairly common in ribs, and spine.
Bone Islands – Plain films • round or ovoid intramedullary sclerotic foci • Do not extend beyond the cortex • The long axis typically parallels the long axis of the involved bone • Homogeneously sclerotic with “thorny” radiating bone spicules that extend from the center of the lesion and blend with the trabeculae • 1 mm to 2 cm in diameter; size generally remains stable
Purpose • The frequency of bone islands has been reported based on plain films only • Where digital workstations are used, bone windows are now routinely reviewed on every CT scan • To determine the frequency of small sclerotic lesions, most probably bone islands, on routine abdominal and pelvic CTs (AP CTs)
Patients and Methods • We prospectively examined AP CT scans of 263 consecutive patients referred over a 6 month period • Patients had no history of neoplastic disease or trauma • Focal sclerotic round or oval lesions in the medulla of the bone were recorded. • Data collected included size, location, and number of lesions per patient.
Patients and Methods For demographic purposes, patients were divided into three age groups: • 40 years or younger • 41-60 years • 61 years or above Data was analyzed for the whole study population as well as for each age group
Results 132 males (50%) 131 females (50%) BI found in 118 pts = 44.8%
Results • A Total of 161 BIs found in 118 pts • single BI - 71% • two BI - 21% • three BI - 8% • Size ranged from 1-13mm (mean 7mm, median 7mm).
Results BI location: iliac bone16.7% acetabulum20.5% sacrum 16.7% femur 27.3% ischium 5.5% vertebrae 8% pubic bone 5%
Conclusion • BI are detected much more commonly on CT than previously reported on plain radiographs – 44.8%
Work in progress • Our study evaluated the incidence of BI in a general population (low risk). • However, these lesions may cause confusion when incidentally found, mostly in oncology patients . • Management guidelines need be established, taking in account their relatively high incidence. • The incidence in an oncologic subset of patients is in evaluation.