Download
1 / 30
320 likes | 846 Views
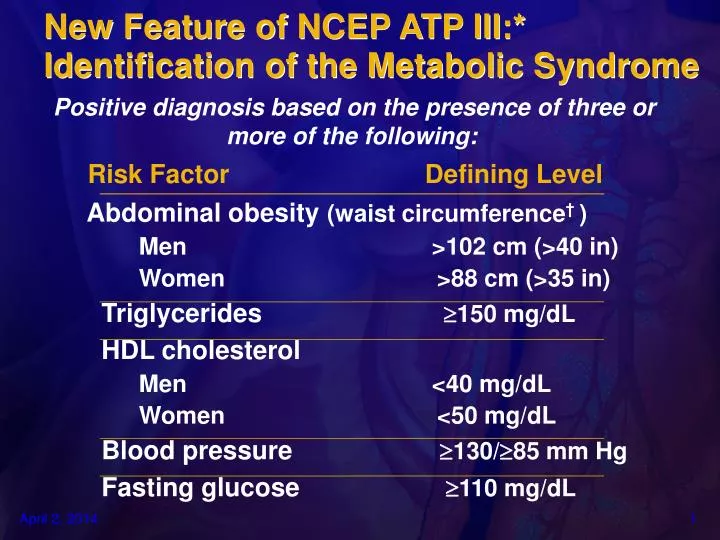
New Feature of NCEP ATP III:* Identification of the Metabolic Syndrome. Positive diagnosis based on the presence of three or more of the following:. Risk Factor Defining Level. Abdominal obesity (waist circumference † )

E N D
New Feature of NCEP ATP III:*Identification of the Metabolic Syndrome Positive diagnosis based on the presence of three or more of the following: Risk Factor Defining Level Abdominal obesity(waist circumference† ) Men >102 cm (>40 in) Women >88 cm (>35 in) Triglycerides 150 mg/dL HDL cholesterol Men <40 mg/dL Women <50 mg/dL Blood pressure130/85 mm Hg Fasting glucose 110 mg/dL
INSULIN RESISTANCE • An impaired biological response to insulin • Resistance to insulin-stimulated glucose uptake • An impairment of normal glucose uptake by muscle • Unregulated overproduction of glucose by the liver • Core defect in T2DM • Underlying defect in the metabolic syndrome (clinical picture)
Visceral obesity is associated with a cluster of metabolic abnormalities
Metabolic Syndrome: Total and CV Mortality in Middle-Aged Men in Kuopio Heart Study Cardiovascular Disease Mortality All-Cause Mortality Metabolic Syndrome Metabolic Syndrome 20 20 Yes RR (85% CI)3.55 (1.96-6.43) RR (85% CI)2.13 (1.64-3.61) 15 15 Cumulative Hazard (%) 10 10 Yes No 5 5 No No. at Risk MetabolicSyndrome 0 0 0 2 4 8 10 12 6 0 2 4 6 8 10 12 Follow-up (Years) Follow-up (Years) Yes 866 852 834 292 No 288 279 234 100 Yes 866 852 834 292 No 288 279 234 100
ROLE OF PEROXISOME PROLIFERATOR-ACTIVATED RECEPTORS • PPARs—Steroid hormone nuclear receptors • Act as ligand-activated transcription factors • Control expression of specific target genes • Protein products control a variety of cellular functions • PPAR-alpha family is a critical regulator of fatty acid metabolism • Expressed throughout vasculature; limits adhesion molecule expression,tissue factor production • PPAR-gamma family plays central role in fatty tissue production,fat metabolism,glucose regulation • Highly expressed in endothelial cells,smooth muscle cells,lymphocytes,macrophages
PPARa regulates Apo A-I, Apo A-II, LPL, ABCA-1 and SR-BI expression
ImpairedInsulinSecretion InsulinDeficiency = GlucoseUptake InsulinResistance = Oral Agents for Type 2 Diabetes: Primary Sites of Action Sulfonylureas Repaglinide Acarbose Miglitol Gut Pancreas CarbohydrateMetabolism Hyperglycemia Hepatic Glucose Production Muscle Liver Rosiglitazone Pioglitazone Metformin
PPAR-GAMMA ACTIVATORS (“glitazones”) • Reduce plaque inflammation • Inhibit expression of adhesion molecules and cytokines • Reduce production of Matrixmetalloproteinases • Reduce thrombogenicity and enhance fibrinolysis • Enhance reverse cholesterol transport and reduce cholesterol content of plaque
Position in Model Variable P Value* First Low-density lipoprotein cholesterol <0.0001 Second High-density lipoprotein cholesterol 0.0001 Third Hemoglobin A1c 0.0022 Fourth Systolic blood pressure 0.0065 Fifth Smoking 0.056 Established Modifiable CV Risk Factors in T2DM UKPDS 23: CAD
Effect of Glycemic Control in the UK Prospective Diabetes Study (UKPDS) Intensive Conventional %Decrease (rate/1000 pt yrs) (rate/1000 pt yrs) Endpoints P Any diabetes related* MI Stroke PVD Microvascular 0.029 0.052 0.52 0.15 0.0099 11 16 – – 25 46 17.4 5 1.6 11.4 40.9 14.7 5.6 1.1 8.6 * Combined microvascular and macrovascular events
Effect of Blood Pressure Control in the UKPDS Tight vs. Less Tight Control • 1,148 Type 2 patients • Average BP lowered to 144/82 mmHg (controls: 154/87); 9-year follow-up Risk Reduction (%) P value Tight Control Any diabetes-related endpoint Diabetes-related deaths Heart failure Stroke Myocardial infarction Microvascular disease 24 32 56 44 21 37 0.0046 0.019 0.0043 0.013 NS 0.0092
UKPDS: Comparison Between Tight Control of BP and Glycemia on Risk of Diabetes Complications Any Diabetes-related Outcome Diabetes-related Death Retino-pathy Micro-vascular Stroke CHF 0 –10 –20 –30 % –40 –50 –60 Tight BP (144/82 vs 154/87 mmHg) Tight glucose (HbA1c 7% vs 7.9%)
Major Outcomes of the Hypertension Optimal Treatment (HOT) Trial: Diabetes Subgroup Diastolic Target p<0.005 <90 mmHg (N=501) <85 mmHg (N=501) <80 mmHg (N=499) Events / 1000 Pt-Years p<0.016 p<0.045 Major CV Events MI CV Mortality Hansson L et al. Lancet 1998;351: 1755-1762.
Heart Outcomes Prevention Evaluation (HOPE) Study Effect of Ramipril on Cardiovascular Events (Myocardial Infarction, Stroke, or CVD Death) ~ 4.5 Yrs 24% RiskReduction 21% RiskReduction 19.8 16.4 15.0 % of Patients 13.0 Placebo Ramipril Placebo Ramipril DiabeticPatients NondiabeticPatients N=3,578, P=<0.001 N=5,719, P=<0.001
Nonfatal MI CV Death Total Mortality Stroke 0 -5 -10 -15 Risk Reduction (%) -20 22% † -25 *P = 0.0074 †P = 0.01 ‡P = 0.0001 §P = 0.0004 24% § -30 -35 33% * -40 37% ‡ MICRO-HOPE: Ramipril Significantly Reduces Cardiovascular Morbidity Ramipril Effects Beyond Baseline Therapy • •Aspirin • • Other Antiplatelet Agents • • Lipid-Lowering Agents • •Diuretics • • Beta-Blockers • • Calcium-Channel Blockers
Angina and Coronary Artery Disease in Patients with Diabetes Mellitus
Evolving Science: Central Role of Ang II in Atherosclerosis Inflammation EndothelialDysfunction Lipid Oxidation IL-5MCP-1PDGF LOX-1 ImpairedNO synthase VCAMICAM Thrombosis Angiotensin II PAI-1TF Adhesion Angiotensin TGF-b ProliferationFibrosis Autostimulation
Antiplatelet Agents Reduce CVD Events in Patients with Diabetes: Antiplatelet Trialists’ Collaboration P<0.002 Antiplatelet Therapy Control P<0.00001 CVD Events (%) Diabetes No Diabetes
CHD Incidence by HbA1c Levels in Type 2 Diabetic Subjects HbA1c tertile Low <6% Middle 6% to 7.9% High >7.9% 25 † 20 Incidence (%) in 3.5 y * 15 10 5 0 All CHD Events CHD Mortality *P<0.01 vs. lowest tertile; †P<0.05 vs. lowest tertile; n=229 men and women. Patients 65–74 years old with T2DM at baseline.
COLLABORATIVE ATORVASTATIN DIABETES STUDY (CARDS) To evaluate the effectiveness and safety of atorvastatin 10mg daily versus placebo in the primary prevention of cardiovascular disease (major coronary events, revascularisation and stroke) in patients with type 2 diabetes without raised cholesterol levels
15 10 5 0 0 1 2 3 4 4.75 CARDS:Cumulative Hazard for Primary Endpoint Relative Risk Reduction 37% (95% CI: 17-52) P=0.001 Placebo 127 events Cumulative Hazard (%) Atorvastatin 83 events Years Placebo 1410 1351 1306 1022 651 305 Atorva 1428 1392 1361 1074 694 328
Event Placebo* Atorva* Hazard Ratio Risk Reduction (CI) Primary endpoint 127 (9.0%) 83 (5.8%) 37% (17-52) p=0.001 Acute coronary events 77 (5.5%) 51 (3.6%) 36% (9-55) Coronary revascularisation 34 (2.4%) 24 (1.7%) 31% (-16-59) Stroke 39 (2.8%) 21 (1.5%) 48% (11-69) CARDS: Treatment Effect on the Primary Endpoint .2 .4 .6 .8 1 1.2 * N (% randomised) Favours Atorvastatin Favours Placebo
PREVENTION OF DIABETIC ATHEROTHROMBOSIS • Aggressive treatment of at-risk patients should be pursued, following the latest guideline recommendations • Lipid lowering reduces clinical events and appears to stabilize plaque • ACE inhibitors reduce clinical events and may have antiatherosclerotic actions • Anti-platelet agents prevent thrombotic events • Glycemic control is effective in reducing risk of microvascular events and coronary events