Download
1 / 51
590 likes | 1.34k Views
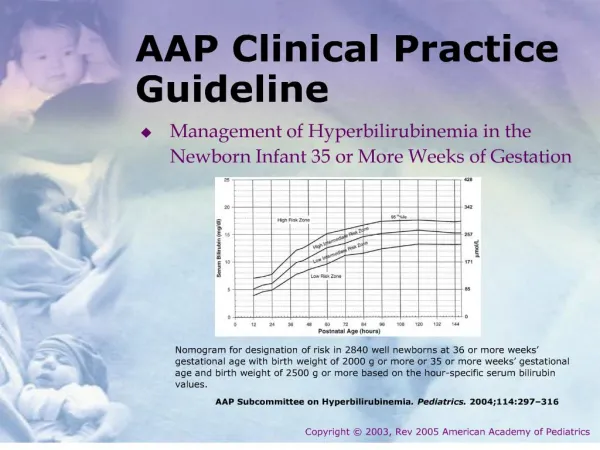
AMDA Clinical Practice Guideline (CPG) for Pain Management. For Medical Directors and Attending Physicians. Introduction to Pain. Pain is common in the long-term care setting. Unrelieved chronic pain is not an inevitable consequence of aging

E N D
AMDA Clinical Practice Guideline(CPG) for Pain Management For Medical Directors and Attending Physicians
Introduction to Pain • Pain is common in the long-term care setting. • Unrelieved chronic pain is not an inevitable consequence of aging • Aging does not increase pain tolerance or decrease sensitivity to pain • Most chronic pain in the long-term care setting is related to arthritis and musculoskeletal problems • Pain may be associated with mood disturbances (for example, depression, anxiety, and sleep disorders)
Introduction to Pain • The use of pain scales • Acute vs. chronic pain • Long-term care interventions
Pain in the Elderly • Definition of Pain—An individual’s unpleasant sensory or emotional experience • Acute pain is abrupt usually abrupt in onset and may escalate • Chronic pain is pain that is persistent or recurrent
Pain in the Elderly • The most common reason for unrelieved pain in the U.S. is failure of staff to routinely assess for pain • Therefore, JCAHO has incorporated assessment of pain into its practice standards • “The fifth vital sign”
Pain in the Elderly Sources of pain in the nursing home Source: Stein et al, Clinics in Geriatric Medicine: 1996
Degenerative joint disease Gastrointestinal causes Fibromyalgia Peripheral vascular disease Rheumatoid arthritis Post-stroke syndromes Low back disorders Improper positioning Pain in the Elderly Conditions Associated with the Development of Pain in the Elderly
Crystal-induced arthropathies Renal conditions Gastrointestinal disorders Osteoporosis Immobility, contracture Neuropathies Pressure ulcers Headaches Amputations Oral or dental Pathology Pain in the Elderly Conditions Associated with the Development of Pain in the Elderly
Different response to pain Staff training Cognitive or sensory impairments Practitioner limitations Social or Cultural barriers System barriers Co-existing illness and multiple medications Pain in the Elderly Barriers to the Recognition of Pain in the LTC setting:
Pain in the Elderly: Myths • To acknowledge pain is a sign of personal weakness • Chronic pain is an inevitable part of aging • Pain is a punishment for past actions • Chronic pain means death is near • Chronic pain always indicates the presence of a serious disease • Acknowledging pain will mean undergoing intrusive and possible painful tests.
Pain in the Elderly: Myths • Acknowledging pain will lead to loss of independence • The elderly – especially cognitively impaired – have a higher pain tolerance • The elderly and cognitively impaired cannot be accurately assessed for pain • Patients in LTC say they are in pain to get attention • Elderly patients are likely to become addicted to pain medications
Pain in the Elderly Consequences of untreated pain: • Depression • Suffering • Sleep disturbance • Behavioral disturbance • Anorexia, weight loss • Deconditioning, increased falls
Pain in the Elderly Inferred Pain Pathophysiology 6] • Nociceptive pain – Explained by ongoing tissue injury • Neuropathic pain – Believed to be sustained by abnormal processing in the peripheral or central nervous system • Psychogenic pain – Believed to be sustained by psychological factors • Idiopathic pain – Unclear mechanisms
AMDA Pain Management CPG—Steps • Recognition • Assessment • Treatment • Monitoring
Pain in the Elderly-Recognition Possible Indicators of Pain in MDS – Version 2.0 • Restlessness, repetitive movements (B5) • Sleep cycle (E1) • Sad, apathetic, anxious appearance (E1) • Change in mood (E3) • Resisting care (E4) • Change in behavior (E5) • Functional limitation in range of motion (G4) • Change in ADL function (G9)
Pain in the Elderly-Recognition Possible Indicators of Pain in MDS – Version 2.0 • Pain site (J3) • Pain symptoms (J2) • Restlessness, repetitive movements (B5) • Sleep cycle (E1) • Sad, apathetic, anxious appearance (E1) • Change in mood (E3) • Resisting care (E4)
Pain in the Elderly-Recognition Possible Indicators of Pain in MDS – Version 2.0 • Loss of sense of initiative or involvement (F1) • Any disease associated with pain (I1) • Pain symptoms (J2) • Pain site (J3) • Mouth pain (K1) • Weight loss (K3)
Pain in the Elderly-Recognition Possible Indicators of Pain in MDS – Version 2.0 • Oral status (L1) • Skin Lesions (M1) • Other skin problems (M4) • Foot Problems (M6) • ROM restorative care (P3)
Pain in the Elderly– Recognition Non-specific signs and symptoms suggestive of pain: • Frowning, grimacing, fearful facial expressions, grinding of teeth • Bracing, guarding, rubbing • Fidgeting, increasing or recurring restlessness • Striking out, increasing or recurring agitation • Eating or sleeping poorly
Pain in the Elderly– Recognition Non-specific signs and symptoms suggestive of pain: • Sighing, groaning, crying, breathing heavily • Decreasing activity levels • Resisting certain movements during care • Change in gait or behavior • Loss of function
Pain Management CPG— Recognition Steps • Is pain present? • Have characteristics and causes of pain been adequately defined? • Provide appropriate interim treatment for pain.
Pain Management CPG— Recognition Pain Intensity Scales for Use with Older Patients – Visual Analogue Scale No painTerrible pain l______l_____l_____l______l_____l______l_____l______l______l 1 2 3 4 5 6 7 8 9 10 Ask the patient:“Please point to the number that best describes your pain” Scale has worst possible pain at a # 10
Pain Management CPG— RecognitionDocumenting an Initial Pain Assessment Pattern: Constant_________ Intermittent__________ Duration: __________ Location: __________ Character: Lancinating____ Burning______ Stinging_____ Radiating______ Shooting_____ Tingling______ Other Descriptors:________________________________ Exacerbating Factors:______________________________ Relieving Factors:_________________________________
Pain Intensity – (None, Moderate, Severe) 1 2 3 4 5 6 7 8 9 10 Worst Pain in Last 24 Hours (None, Moderate, Severe) 1 2 3 4 5 6 7 8 9 10 Mood: ________________________________________ Depression Screening Score: ______________________ Impaired Activities: ______________________________ Sleep Quality: __________________________________ Bowel Habits: __________________________________ Other Assessments or Comments:__________________ ______________________________________________ ______________________________________________ Most Likely Causes Of Pain: _______________________ ______________________________________________ Plans: ________________________________________ ______________________________________________
Pain Management– Assessment Steps • Perform a pertinent history and physical examination • Identify the causes of pain as far as possible • Perform further diagnostic testing as indicated • Identify causes of pain • Obtain assistance/consultations as necessary • Summarize characteristics and causes of the patient’s pain and assess impact onfunction and quality of life
Pain Management– Assessment Steps Pain History [7] – Important Elements to Include: • Known etiology and treatments – previous evaluation, pain diagnoses and treatments • Prior prescribed and non-prescribed treatments • Current therapies
Pain Management– Assessment StepsChronic Pain History “PQRST” • Provocative/palliative factors (e.g., position, activity, etc.) • Quality (e.g., aching, throbbing, stabbing, burning) • Region (e.g., focal, multifocal, generalized, deep, superficial) • Severity (e.g., average, least, worst, and current) • Temporal features (e.g., onset, duration, course, daily pattern) Medical History • Existing comorbidities • Current medications Source: Valley, MA. Pain measurement. In: Raj PP. Pain Medicine. St. Louis MO. Mosby, Inc. 1996:36-46.
Pain Management– Treatment Steps • Adopt an interdisciplinary care plan • Set goals for pain relief • Implement the care plan
Pain Management– Treatment Steps Provide a Comforting and Supportive Environment – • Reassuring words/touch • Topical or low-risk analgesic • Talk with patient/caregivers about pain • Back rub, hot or cold compresses • Whirlpool, shower • Comforting music • Chaplain services
Pain Management– Treatment StepsEthics and Pain • The old ethic of under-prescribing “just say no” “it hurts so good” • The new ethic trust: believing what patients say commitment: formalized mutual agreement standardized care: guidelines on assessment and treatment collaboration: working together Source: Marino A. J Law, Med Ethics, 2001
Pain Management– Treatment General Principles for Prescribing Analgesics in the Long-Term Care Setting • Evaluate patient’s overall medical condition and current medication regimen • Consider whether the medical literature contains evidence-based recommendations for specific regimens to treat identified causes • For example, acetaminophen for musculoskeletal pain; narcotics may not help fibromyalgia • In most cases, administer at least one medication regularly (not PRN)
Pain Management– Treatment General Principles for Prescribing Analgesics in the Long-Term Care Setting • Use the least invasive route of administration first • For chronic pain – begin with a low dose and titrate until comfort is achieved • For acute pain – begin with a low or moderate dose as needed and titrate more rapidly • Reassess/adjust the dose to optimize pain relief while monitoring side effects
Pain Management– Treatment Appropriateness of regular or PRN dosing: • Intermittent/less severe pain – Start with PRN then switch to regular if patient uses more than occasionally. Start with a lower regular dose and supplement with PRN for breakthrough pain. Adjust regular dose depending on frequency/severity of breakthrough pain.
Pain Management– Treatment Appropriateness of regular or PRN dosing • More severe pain Standing order for more potent, longer-acting analgesic and supplement with a shorter acting analgesic PRN • Severe/recurrent acute or chronic pain Regular, not PRN dosage of at least one medication – Start with low to moderate dose, thentitrate upwards
Pain Management– Treatment • Goal of treatment is to decrease pain, improve functioning, mood and sleep • Strength of dosage should be limited only by side effects or potential toxicity
Pain Management CPG– Treatment Non-Opioid Analgesics Used in the Long-Term Care Setting
Pain Management CPG– Treatment Opioid Therapy: Prescribing Principles and Professional Obligations [9] • Drug Selection • Dosing to optimize effects • Treating side effects • Managing the poorly responsive patient
Pain Management CPG– TreatmentOpioid Analgesics Used in the Long-Term Care Setting (Oral and Transdermal)
Pain Management CPG– Treatment * Duration of effect increases with repeated use due to cumulative effect of drug
Pain Management CPG– TreatmentOral Morphine to Transdermal Fentanyl* NOTE : This table is designed to convert from morphine to transdermal fentanyl and is based on a conservative equianalgesic dose. Using this table to convert from transdermal fentanyl to morphine could lead to overestimation of dose.
Counterirritants (menthol, methyl salicylate) Supplied as liniments, creams, ointments, sprays, gels or lotions May be effective for arthritic pain (not multiple joint pain) Capsaicin cream (0.025%) and (0.075%) Derived from red peppers Depletes substance P, desensitizes nerve fibers associated with pain Main limitations are skin irritation and need for frequent application Need to use routinely for optimal effectiveness TreatmentTopical Analgesics
Chronic use of the following drugs are notrecommended: Indomethacin Piroxicam Tolmetin Meclofenamate Propoxyphene Meperidine Pentazocine, butorphanol and other agonist-antagonist combinations TreatmentAnalgesics of Particular Concern in the Long-Term Care Setting
Neuropathic pain Antidepressants Anticonvulsants Antiarrhythmics Baclofen Inflammatory diseases Corticosteroids Osteoporotic fractures Calcitonin Treatment Non-Analgesic Drugs Sometimes Used for Analgesia
Treatment Factors to evaluate when considering complementary therapies • Patient’s underlying diagnosis and co-existing conditions • Effectiveness of current treatment • Preferences of the patient and family or advocate • Past patient experience with the therapy • Availability of skilled experienced providers
Pain Management CPG– Monitoring Steps • Re-evaluate the patient’s pain • Adjust treatment as necessary • Repeat previous steps until pain is controlled
Pain Management CPG– MonitoringOpioid Therapy: Monitoring Outcomes Critical outcomes: The “Four A’s” • Analgesia – Is pain relief meaningful? • Adverse events – Are side effects tolerable? • Activities - Has functioning improved? • Aberrant drug-related behavior
Pain Management CPG– Monitoring When patient is unresponsive to clinical management consider referral to: • Geriatrician • Neurologist • Physiatrist • Pain clinic • Physician certified in palliative medicine • Psychiatrist (if patient has co-existing mood disorder)
Dilemmas in Pain Management While addressing pain management, have strategies in mind for common problems • Patient refusal of potentially beneficial medication • Patient and family pressure to prescribe certain drugs • Patient and family misconceptions about illness • Unrecognized or denied psychiatric disturbances
Reviewing the Physician’s Role • Prevention strategies • Communication with patients/families • Documentation • Participate in Quality Improvement • Follow policies and procedures