Download
1 / 36
370 likes | 564 Views
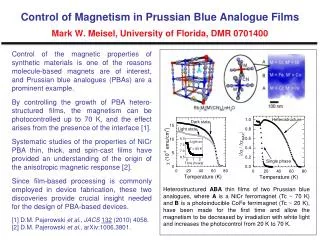
Venice 9 nov 2006: HuGE-Network of Networks. Assessment of biological plausibility: osteoporosis. A ndré G Uitterlinden Genetic Laboratory Department of Internal Medicine Department of Epidemiology&Biostatistics Department of Clinical Chemistry. Molecular Genetic Epidemiology.

E N D
Venice 9 nov 2006: HuGE-Network of Networks Assessment of biological plausibility: osteoporosis André G Uitterlinden Genetic Laboratory Department of Internal Medicine Department of Epidemiology&Biostatistics Department of Clinical Chemistry
Monogenic mutation model Genome Wide Linkage Genome Wide Association Candidate gene association humans mice humans mice humans humans *Chromosomal region x x x x *Gene x x x x x LD block x x Haplotype alleles x x variant x x x x Osteoporosis Genetics: alignement of evidence * Genetic: Type of evidence Genetic resolution * Functional: mRNA, protein, cells, etc
Determine “Functional” Effects of DNA Polymorphisms DNA polymorphism Organizational Level “Read-out” of functionality mRNA -level, stability, splicing/isoforms Protein -level, stability, isoforms, protein-protein Cells-e.g., transcriptional activity -e.g., Cell growth inhibition Humans -Serum parameters -Intervention Association with disease: > 70 yrs follow-up !
IGFI, IGFBP3 GR, 11B-HSD Cortisol IGF/GH TSHR, DIO1, DIO2, DIO3, MCT8 Thyroid Hormone ERα, ERβ, Aromatase, LH, LHR, GnRH VDR,DBP Vitamin D Estrogen Genetic determinants of osteoporosis ? TGFb/BMP/Wnt-signalling homocysteine Matrix molecules MTHFR, MS, MTRR, CBS, THYMS TGFb,LRP5/6, BMP2, FRZB, SOST Collagen Ia1, osteocalcin, AHSG, LOX
Examples • Lipoprotein-related Receptor 5 (LRP5; 11q12) • (van Meurs et al, JBMR 2006) • Collagen type IA1 (COLIA1; 17q22) • (Uitterlinden et al, New Engl J Med 1998; Ralston et al., PLoS Medicine 2006) • Estrogen Receptor alpha (ESR1; 6q25) • (van Meurs et al, Hum Mol Genet 2003; Ioannidis et al., JAMA 2004) • Vitamin D Receptor (VDR; 12q13) • (Fang et al, Am J Hum Genet 2005; Uitterlinden et al., Ann Int Med, in press)
A locus for high BMD and low BMD on the same region of chromosome 11q12-13 HBM Family D11S905 D11S987 D11S937 7.0 OPS linkage 5.0 LOD 3.0 Osteoporosis Pseudoglioma Syndrome 1.0 HBM linkage Gong et al. AJHG 1996 Johnson et al. AJHG 1997 Chr 11
High Bone Mass: • Several activating mutations • All affect first “propeller” motif of LRP5 Different LRP5 mutations cause osteoporosis pseudoglioma and high bone mass A214T A214V G171R D111Y A242T T253I W10X R428X R570W D718X Q853X E1270fs V667M W734X D490fs D769fs R494Q • Osteoporosis-pseudoglioma Syndrome • Homozygous (recessive) mutations • Cause loss of receptor function Gong et al Cell 2001 Little et al AJHG 2002 Wesenbeeck et al AJHG 2003
LRP5 Ala1330Val and LRP6 Ile1062Val polymorphisms Wnt/Frizzled Interaction YWTD spacer motif DKK Interaction I1062V EGF-like domain A1330V LDLR-like binding domain
Bone phenotypes throughout life: LRP5 Val1330 associated with low BMD in boys and males -Koay et al, JBMR 2004 -van Meurs et al, JBMR 2006 -Ferrari et al, AJHG 2004 (Hartikka et al, JBMR 2005) Peak BMD Bone Loss Bone growth Osteoporosis: Low BMD, fractures men BMD women 75 25 50 100 Age (yr)
Examples • Lipoprotein-related Receptor 5 (LRP5; 11q12) • (van Meurs et al, JBMR 2006) • Collagen type IA1 (COLIA1; 17q22) • (Uitterlinden et al, New Engl J Med 1998; Ralston et al., PLoS Medicine 2006) • Estrogen Receptor alpha (ESR1; 6q25) • (van Meurs et al, Hum Mol Genet 2003; Ioannidis et al., JAMA 2004) • Vitamin D Receptor (VDR; 12q13) • (Fang et al, Am J Hum Genet 2005; Uitterlinden et al., Ann Int Med, in press)
Type I collagen, osteogenesis imperfecta and the genetics of osteoporosis collagen • Collagen is the major protein of bone • Proteins encoded by COLIA1 and COLIA2 genes • Collagen genes produce alpha 1 and alpha 2 chains • Chains assemble to form collagen fibres • Mutations in collagen coding regions cause extreme bone fragility and severe osteoporosis • “brittle bone disease” • osteogenesis imperfecta (OI) “blue” eyes in OI fractures in OI
Genotype frequency G/G:70% G/T: 25% T/T: 5% Allele frequency: G: 80% T: 20% The polymorphic Sp1 binding site in the Collagen type I alpha 1 gene +1240 +1260 Sp1 G -------GGGAATG GGGCGGGAT GAGGGCT---- T COL1A1 Locus: 17q21.31-q22.05 Exon 1 Exon 2 Sp1 sites T-allele: -Sp1 binding ↑ -mRNA expression ↑ Grant et al., Nature Genetics, 1996
60 50 40 30 20 10 0 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 COL1A1Sp1 polymorphism affects mechanical strength of bone Take cores from femoral head bone biopsies Energy Input (Kj/m3) p<0.03 Mechanical testing GG GT Yield Density (g/cm3) Stress (Mpa) NSD Energy Strain (%) Mann et al, JClinInvest 2001 GG GT
Sp1 binding COLIA1 transcription Mechanisms of bone fragility in subjects with COL1A1 Sp1 T-allele ColIA1: T-allele ColIA1: G-allele colIA2 + colIA2 a1(I) chain overproduced + a 1 (I) homotrimer a 1 (I) homotrimer alters packing of collagen? Normal cross linking of collagen heterotrimers Increased bone fragility
GENOMOS meta-analysis: COLIA1 Genotype and Fracture (Ralston, Uitterlinden,…..Ioannidis; PLoS Medicine 2006) *OR inc vert fx: TT vs GT+GG = 1.33 [CI 1.00-1.77] * FN and LS BMD 0.02 g/cm2 lower for TT homozygotes
COLLAGEN IA1 Sp1 G to T POLYMORPHISM fiction or function ? • SUPPORTING EVIDENCE: • Epidemiological evidence for T-allele: • - Meta-analyses: Association of T-allele with lower BMD and increased fx-risk • Molecular biological / cell biological evidence for T-allele: • - Cell biological studies: ↑ mRNA, ↑ protein, ↓ Ca-deposition • - Bone biopsy studies: ↓ bone strength • - Mouse model (oim/oim mouse: lacks COLIa2) is in support • Conclusion: • The COLIA1 Sp1 polymorphism is functional • - The COLIA1 Sp1 T-allele is a susceptibility allele for osteoporosis but with small effect of only the TT homozygotes
Examples • Lipoprotein-related Receptor 5 (LRP5; 11q12) • (van Meurs et al, JBMR 2006) • Collagen type IA1 (COLIA1; 17q22) • (Uitterlinden et al, New Engl J Med 1998; Ralston et al., PLoS Medicine 2006) • Estrogen Receptor alpha (ESR1; 6q25) • (van Meurs et al, Hum Mol Genet 2003; Ioannidis et al., JAMA 2004) • Vitamin D Receptor (VDR; 12q13) • (Fang et al, Am J Hum Genet 2005; Uitterlinden et al., Ann Int Med, in press)
VITAMIN D RECEPTOR GENE Chromosome 12q13 > 102 kb 1f 1e 1a 1d 1b 1c 2 3 4,5,6 7,8,9,UTR Bsm, Apa, Taq Cdx2 Fok The first “osteoporosis gene” to be studied (Morrison et al, 1994), but.... a complex gene with many polymorphisms.......
VDR Sequencing Results: Fang et al., Am J Hum Genet 2005 Nejentsev et al., Hum Mol Genet 2005
LD Map of 34 SNPs in the VDR Gene (234 Caucasian subjects) Fang et al., Am J Hum Genet 2005
1 2 3 4 5 Polymorphisms and Haplotype Map of the VDR Gene in Caucasians Haplotype blocks Fang et al., Am J Hum Genet 2005
VDR Cdx-2 polymorphism (Yamamoto et al., JBMR 1999; Arai et al, JBMR 2000) • SNP in a binding site for transcription factor Cdx-2 • Cdx-2 protein plays an important role in the small intestine-specific transcription of VDR
VDR Cdx-2 SNPinfluences VDR promoter function Arai et al. J Bone Miner Res 2001 Differences in; • gel-shift assays • reporter gene expression • A-allele has higher transcriptional activity than G-allele
association analysis: BMD by VDR Cdx-2 genotype (in Japanese women: Arai et al. JBone Miner Res, 2001) VDR Cdx-2 genotype is associated with BMD: A-allele associated with higher lumbar spine BMD in 45 postmenopausal Japanese women, but not in 68 premenopausal women
GENOMOS meta-analysis: Cdx2 VDR Genotype and Vertebral Fracture (Uitterlinden, Ralston…..Ioannidis; Ann Int Med 2006)
1 2 3 4 5 Polymorphisms and Haplotype Map of the VDR Gene in Caucasians Haplotype blocks Fang et al., Am J Hum Genet 2005
Different alleles between Hap_u1 & u2 of the VDR 3’-UTR 933 1200 1851 2689 3206 U-A311C U-796delT U-A1909C U-2119(A)13-24 U-T2147A hap_u1 =baT (40%) C T C AL A hap_u2 =BAt (39%) A - A AS T Fang et al., Am J Hum Genet 2005
Transfection of VDR 3’UTR Haplotype Different UTR variants: hap_u1, u2, u3, u4 & empty vector Transfection in different cell-lines (24 hrs) RNA isolated at: 0, 8 16, 24 and 32 hrs (after inhibition of transcription) UTR 1 2 3 4 RT-PCR & real-time PCR: -VDR -Neomycin (transfection efficacy)
Neo-normalized VDR mRNA Levels by VDR 3’-UTR haplotypes in cell-lines Fang et al. AJHG 2005
Vit D other haplotypes VDR Hap1 of block2 (Hap3 of block3) Hap1 of block5
GENOMOS meta-analysis: VDR Genotype and Any Fracture (Uitterlinden, Ralston…..Ioannidis; Ann Int Med 2006)
Pleiotropic effects of a risk gene Schuit et al., J Clin Endcrinol. Metab., 2004 Height Bergink et al., Arth&Rheum, 2003 Osteoarthritis E2 levels Myocardial Infarction ERα PvuII/XbaI polymorphisms Schuit et al., submitted Schuit et al., JAMA, 2004 Hysterectomy Weel et al., J Clin Endocrinol.Metab., 1999 Stroke Amygdalar volume Schuit et al., submitted Age at Menopause Weel et al., J Clin Endocrinol.Metab., 1999 den Heijer et al., Mol.Psych. 2004 Ioannidis et al., JAMA, 2004 van Meurs et al., Hum Mol Genet., 2003 Colin et al., J Clin Endocrinol. Metab., 2003 Osteoporosis Anxiety Tiemeyer et al., Mol Psych, in press
Determine “Functional” Effects of DNA Polymorphisms DNA polymorphism Organizational Level “Read-out” of functionality mRNA -level, stability, splicing/isoforms Protein -level, stability, isoforms, protein-protein Cells-e.g., transcriptional activity -e.g., Cell growth inhibition Humans -Serum parameters -Intervention Association with disease: > 70 yrs follow-up !
Why is the study of polymorphisms important ? Disease Evolution Forensics This is what happens when there are NO POLYMORPHISMS Slide stolen from Dr Axel Themmen