Download

1 / 27
720 likes | 3.24k Views
Graft Versus Host Disease. Criteria for Development of GVHD. Graft contains immunologically competent cells Host appears foreign to the graft; it has alloantigens that are capable of antigenically stimulating the graft

E N D
Criteria for Development of GVHD • Graft contains immunologically competent cells • Host appears foreign to the graft; it has alloantigens that are capable of antigenically stimulating the graft • Host is unable to mount an effective immunological reaction against the graft
Patients at High Risk for GVHD • Allogeneic & autologous hematopoietic cell transplantation (age, HLA disparity, gender disparity, allosensitized donor) • Solid organ transplantation (liver, small bowel) • Transfusion of unirradiated blood products (fetuses, neonates, immunodeficiency syndromes, chemoradiotherapy)
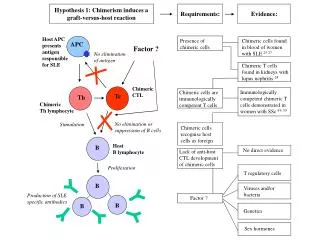
Pathophysiology of GVHD – 3 stages • Damaged host tissue cytokines (TNFα, IL1) stimulate APCs recognition of host Ag by donor T cell • Donor T cell activated cytokines (IFNγ, IL2) induce CTL, NKC, phagocytes • Phagocytes release more cytokines cell lysis/apoptosis tissue destruction
2 Types of GVHD • Acute (10-30 days posttransplant) - triad of derm, hepatic, and GI manifestations (barriers to infection thus APCs) - 40-80% incidence (depends on HLA match) • Chronic ( >100 days posttransplant) - diverse range of affected organ systems - 70-90% evolve from acute GVHD - 20% occur de novo - 10% occur after acute GVHD resolves
Acute GVHD – Dermatological • Painful or pruritic erythematous macules of palms, soles, trunk, limbs • Confluent erythema, erythroderma and/or papule formation • Subepidermal bullae and vesicle formation • Stages 1-4 based on % BSA involved and presence of bullae/vesicles
Acute GVHD – Dermatological • Boy who developed stage 3 skin involvement with acute graft versus host disease despite receiving prophylaxis with cyclosporin A. The donor was a sister matched for human leukocyte antigen. The gender disparity increased the risk for acute graft versus host disease.
Acute GVHD – Hepatic • Asymptomatic elevations in bilirubin, ALT, AST, alkaline phosphatase similar to cholestatic jaundice
Acute GVHD – GI • Anorexia • Dyspepsia • Cramping abdominal pain • Diarrhea (secretory diarrhea may persist despite NPO) • Intestinal bleeding • Ileus
Chronic GVHD - Dermatological • Same as acute GVHD • Atrophy and erythema of oral mucosa • Lichenoid lesions of skin, buccal and labial mucosa • Sclerodermatous skin thickening • Joint contractures
Chronic GVHD – Ocular • Keratoconjunctivitis sicca may lead to corneal erosions • Hemorrhagic conjunctivitis • Pseudomembrane formation • Lagophthalmos
Chronic GVHD – Pulmonary • Obstructive lung disease • Dyspnea, wheezing, chronic cough • Nonresponsive to bronchodilators • Bronchiolitis obliterans
Chronic GVHD – GI • Same as acute GVHD • Sensitivity to acidic or spicy foods • Odyno/Dysphagia • Esophageal strictures or dysmotility • Weight loss
Chronic GVHD – Hepatic • Same as acute GVHD • Hyperbilirubinemia – jaundice, pruritis and excoriations • Portal HTN, cirrhosis, and hepatic failure are rare
Chronic GVHD – Neuromuscular • Weakness • Neuropathic pain • Muscle cramps • Symptoms may resemble myasthenia gravis or polymyositis
Chronic GVHD – Misc. • Many similarities to autoimmune disorders • SLE • Sjogren syndrome • Rheumatoid arthritis • Primary biliary cirrhosis • Lichen planus
Prevention • Depletion of T cells from donor has reduced the incidence of GVHD, however, this results in increased incidence of graft failure and malignancy occurrence • Leukemic cells may have specific antigen profiles that make them susceptible to the GVL effect.
Graft vs. Leukemia Effect • Mortality of GVHD with no leukemic relapse vs. mortality of leukemic relapse and no GVHD is under investigation
Prophylactic Treatment • Cyclosporine (CSP) + Methotrexate (MTX) +/- Prednisone 180 days • Tacrolimus (Prograf) + MTX 180 days • IVIG for antibody prophylaxis Qweek x12 (good for acute , not chronic)
Primary Treatment for Acute GVHD • CSP or Prograf + methylprednisolone (MP) • Antihymocyte globulin (ATG) • Mycophenolate mofetil (CellCept) • Anti-CD5 immunotoxin • XomaZyme – pan T cell immunotoxin
Secondary Treatment for Acute GVHD • ATG • Increased MP doses • Muromonab-CD3 • IL-1 receptor antagonist • Conversion from CSP to Prograf • Psoralen +UVA light (PUVA) for cutaneous GVHD
Primary Treatment for Chronic GVHD • Prednisone 1 mg/kg QOD +/- CSP • Thalidomide
Secondary Treatment for Chronic GVHD • Azathioprine (Imuran) • Alternating CSP & Prednisone • Thalidomide • Clofazimine (antileprosy agent) and PUVA for cutaneous GVHD
Prognosis • Acute GVHD: response to tx 25% mortality vs. 75% mortality with no response or progression. • Chronic GVHD: 6 yr. mortality is 58% overall and 90% for progressive disease. • Mortality for both acute and chronic GVHD is mostly due to sepsis. • Higher mortality in patients with HLA mismatched donor, bilirubin > 2 mg/dL, thrombocytopenia, lichenoid skin histology, high dose prednisone.
References • Fleming DR, Graft-vs-host disease: what is the evidence? Evidence-based Oncology 2002; 3. • Mandanas RA, et al. Graft versus host disease. Emedicine.com/med/topic926. • Hoffman: Hematology: Basic Principles and Practice, 3rd ed., 2000. • Kuechle MK, et al. Graft versus host disease. Emedicine.com/derm/topic478.