Download
1 / 29
290 likes | 605 Views
Lichenoid eruptions. Lichen Planus. Description Flat-topped, polygonal, violaceous papules and plaques Wickham’s striae : fine lacy pattern Dorsal surface of extremities Koebner phenomenon at sites of trauma Nail dystrophy Oral mucosa: lacy white plaques. Lichen Planus. Treatment

E N D
Lichen Planus • Description • Flat-topped, polygonal, violaceous papules and plaques • Wickham’s striae: fine lacy pattern • Dorsal surface of extremities • Koebner phenomenon at sites of trauma • Nail dystrophy • Oral mucosa: lacy white plaques
Lichen Planus • Treatment • Topical steroids • Course • Prolonged period of hyperpigmentation can be expected
Lichen Striatus • Description • Flat-topped papules appear abruptly • Erythematous or hypopigmented • Surfaces with fine scale • Linear or swirled distribution • (along skin lines of Blaschko) • Nail dystrophy • Location • Extremeties, neck, upper back
Lichen Striatus • Timing • Peak in school-age children • Course • Spontaneous resolution 1-2yrs
Tzanck Smear • Tells you that it’s a viral lesion • Multinucleated giant cell • Not specific to type of virus • Outdated • Use DFA, PCR, or Viral culture
Blistering Distal Dactylitis • Superficial bacterial skin infection • Cause: GAS, GBS, S.aureus • Location • Tips of pads of fingers/toes • Description • Tense blisters, 5-10mm • Filled with thin, purulent fluid • Narrow erythematous rim • Thick crust upon rupture
Question 3 • Which is true of the condition pictured? • A Use of systemic steroids may improve survival • B Systemic antibiotics with G+ coverage are the mainstay of treatment • C Permanent sequelae may include visual impairment • D Nikolsky’s sign is negative
Erythema Nodosum • Description • Symmetrical, red, tender nodules • 1-5cm • Location • Pretibial • Hypersensitivity reaction, associated with: • Strep • Sarcoid • Ulcerative colitis • TB • Other bacterial/fungal infxn • Oral contraceptives and other meds
Erythema Nodosum • Timing/Course • >10y/o • Lasts 2-6wks • Often recurs • Description • Red, tender, slightly elevated nodules • Indurated SQ plaques • Brownish-red or purplish-red hue • Shins most common site • Treatment • Tx underlying cause • Pain: NSAIDS and rest
Urticaria • Aka “Hives” “Welts” • Course • Sudden onset • Transient • Lasts 1-24hrs • Description • Well-demarcated intensely pruritic • Appear to migrate • May coalesce • White/red “halo”
Urticaria • Cause: can be IgE or complement mediated • Acute (<6wks) • IgE • Acute infections (strep, mono) • Foods • Drugs • Insect bites • Contact or inhaled allergen • Chronic (>6wks) • Occult infection • Hep B • Connective tissue dz
Question 4 • This child has mild edema of hand/feet and painful migratory periarticular swelling of wrists and ankles. The most likely etiology is: • A Staph Scalded Skin Syndrome • BHenoch-Schonlein Purpura • C Hemolytic Uremic Syndrome • D Interstitial nephritis as part of a reaction to medications • E Serum Sickness-Like Reaction
Serum Sickness-Like Reaction • Type III reaction: Immune-Complex Deposition • Symptoms • Urticarial lesions • Relatively nonpruritic • Target or serpiginous • Periarticular swelling • Migratory • Stocking-glove angioedema • Painful • Facial edema • Fever
Serum Sickness-Like Reaction • Triggers • URI • Meds • Sulfa • Cefaclor • Minocycline • PCN • Course • Wax and wane over 1-3wks
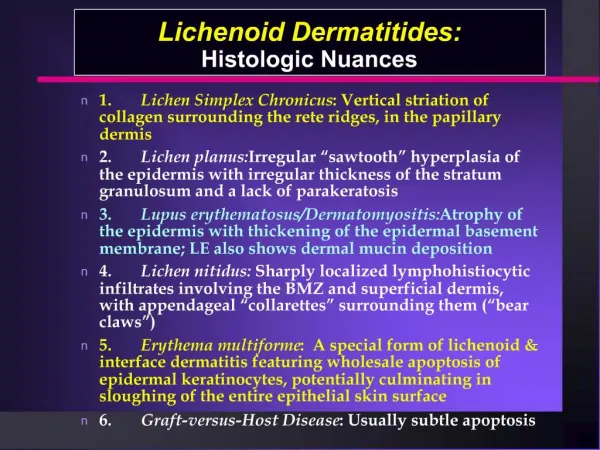
ErythemaMultiforme • Hypersensitivity syndrome • Causes • Drugs, viruses, bacteria, foods, immunizations • Connective tissue dz • Recurrent EM • Recurrent HSV infxn • Location • Any part of body • Commonly: palms/soles, arms/legs
ErythemaMultiforme • Description • Symmetrical • Dusky red macules – evolve into iris or target-shaped lesions • Center of target may be blue, violaceous, or white • Vescicles or bullae may develop • Center or ring of target • May appear as diffuse urticaria initially • Non-pruritic, may be painful
ErythemaMultiforme • Course • Crops last 1-3 wks • Self limited • ?Mild systemic symptoms? • Low grade fever • Malaise • Myalgia • Mucous membranes spared • Or mildly involved
SJS / TEN • Epidermal and mucous membrane necrosis and sloughing • Cleavage beneath basment membrane zone • Full-thickness sloughing • SJS: <30% BSA • TEN: >30% BSA • Cause: hypersensitivity, viral infxn, connective tissue dz, malignancy
SJS/TEN Complications • Ophtho: • Corneal scarring • Lid scarring: ectropion • FEN • Dehydration • Malnutrition • Electrolyte imbalance • ID • Superficial infection • Sepsis • Death
SJS / TEN • Treatment • IVIG • Steroids relatively contraindicated • GI symptoms • Immune suppression • Differentiate from SSSS • SSSS • Bullae more thin-walled • Mucous membranes red, but do not slough
Morbilliform Drug Eruption • 75% of all cutaneous drug reactions • Description • Erythematousmacules and papules • Range from fine to blotchy • Eruption 5-14days after starting med • Face/Trunk extremities • May become confluent • Resolves over 1-2 wks • May see mild purpura, desquamation
Fixed drug eruption • Recur at same localized site following reexposure to offending drug • Target and bullous lesions • Resemble erythemamultiforme • Morphologically and histologically • (only localized)
Henoch-SchonleinPurpura • Classic Tetrad • Palpable purpura • Without thrombocytopenia or coagulopathy • Present in almost all patients • Arthritis/Arthralgia • 75% • Abdominal Pain (May have hematochezia) • 50% • Intussussception (ileo-ileal) • Renal Disease (Mild) • 21-54% • Not all symptoms must be present for diagnosis • Takes days to weeks to develop • May present as abd pain or joint complaints* • May recur
Henoch-SchonleinPurpura • Diffuse Vasculitis • Histo: • immune-complex deposition in capillaries • Leukocyticvasculitis in skin • Treatment • Supportive • May use steroids if severe
Henoch-SchonleinPurpura • DIFFERENTIATE FROM HUS • Hemolytic Uremic Syndrome • More toxic • Renal involvement more severe (dialysis) • Hemolytic: anemia, thrombocytopenia • More severe neuro manifestations