Download
1 / 1
10 likes | 149 Views
Fidelity to Manualized Psychotherapy: Integration of Research Methods in Mental Health Clinical Training Weronika Micula-Gondek MD, Jennifer Levin PhD, Martha Sajatovic MD Department of Psychiatry, University Hospitals Case Medical Center, Cleveland, Ohio. Results

E N D
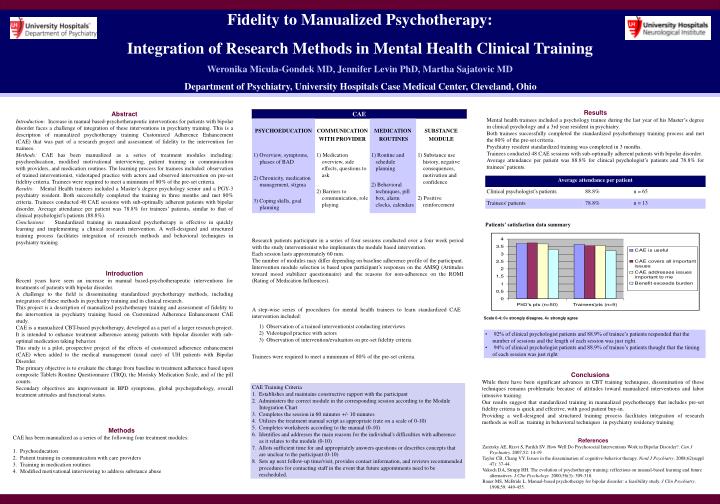
Fidelity to Manualized Psychotherapy: Integration of Research Methods in Mental Health Clinical Training Weronika Micula-Gondek MD, Jennifer Levin PhD, Martha Sajatovic MD Department of Psychiatry, University Hospitals Case Medical Center, Cleveland, Ohio Results Mental health trainees included a psychology trainee during the last year of his Master’s degree in clinical psychology and a 3rd year resident in psychiatry. Both trainees successfully completed the standardized psychotherapy training process and met the 80% of the pre-set criteria. Psychiatry resident standardized training was completed in 3 months. Trainees conducted 48 CAE sessions with sub-optimally adherent patients with bipolar disorder. Average attendance per patient was 88.8% for clinical psychologist’s patients and 78.8% for trainees’ patients. Abstract Introduction: Increase in manual based-psychotherapeutic interventions for patients with bipolar disorder faces a challenge of integration of these interventions in psychiatry training. This is a description of manualized psychotherapy training Customized Adherence Enhancement (CAE) that was part of a research project and assessment of fidelity to the intervention for trainees. Methods: CAE has been manualized as a series of treatment modules including: psychoeducation, modified motivational interviewing, patient training in communication with providers, and medication routines. The learning process for trainees included: observation of trained interventionist, videotaped practice with actors and observed intervention on pre-set fidelity criteria. Trainees were required to meet a minimum of 80% of the pre-set criteria. Results: Mental Health trainees included a Master’s degree psychology senior and a PGY-3 psychiatry resident. Both successfully completed the training in three months and met 80% criteria. Trainees conducted 48 CAE sessions with sub-optimally adherent patients with bipolar disorder. Average attendance per patient was 78.8% for trainees’ patients, similar to that of clinical psychologist’s patients (88.8%). Conclusions: Standardized training in manualized psychotherapy is effective in quickly learning and implementing a clinical research intervention. A well-designed and structured training process facilitates integration of research methods and behavioral techniques in psychiatry training. Patients’ satisfaction data summary Research patients participate in a series of four sessions conducted over a four week period with the study interventionist who implements the module based intervention. Each session lasts approximately 60 min. The number of modules may differ depending on baseline adherence profile of the participant. Intervention module selection is based upon participant’s responses on the AMSQ (Attitudes toward mood stabilizer questionnaire) and the reasons for non-adherence on the ROMI (Rating of Medication Influences). Introduction Recent years have seen an increase in manual based-psychotherapeutic interventions for treatments of patients with bipolar disorder. A challenge to the field is disseminating standardized psychotherapy methods, including integration of these methods in psychiatry training and in clinical research. This project is a description of manualized psychotherapy training and assessment of fidelity to the intervention in psychiatry training based on Customized Adherence Enhancement CAE study. CAE is a manualized CBT-based psychotherapy, developed as a part of a larger research project. It is intended to enhance treatment adherence among patients with bipolar disorder with sub-optimal medication taking behavior. This study is a pilot, prospective project of the effects of customized adherence enhancement (CAE) when added to the medical management (usual care) of UH patients with Bipolar Disorder. The primary objective is to evaluate the change from baseline in treatment adherence based upon composite Tablets Routine Questionnaire (TRQ), the Morisky Medication Scale, and of the pill counts. Secondary objectives are improvement in BPD symptoms, global psychopathology, overall treatment attitudes and functional status. A step-wise series of procedures for mental health trainees to learn standardized CAE intervention included: 1) Observation of a trained interventionist conducting interviews 2) Videotaped practice with actors 3) Observation of intervention/evaluation on pre-set fidelity criteria Trainees were required to meet a minimum of 80% of the pre-set criteria. Scale 0-4; 0= strongly disagree, 4= strongly agree • 92% of clinical psychologist patients and 88.9% of trainee’s patients responded that the number of sessions and the length of each session was just right. • 94% of clinical psychologist patients and 88.9% of trainee’s patients thought that the timing of each session was just right Conclusions While there have been significant advances in CBT training techniques, dissemination of those techniques remains problematic because of attitudes toward manualized interventions and labor intensive training. Our results suggest that standardized training in manualized psychotherapy that includes pre-set fidelity criteria is quick and effective, with good patient buy-in. Providing a well-designed and structured training process facilitates integration of research methods as well as training in behavioral techniques in psychiatry residency training CAE Training Criteria 1. Establishes and maintains constructive rapport with the participant 2. Administers the correct module in the corresponding session according to the Module Integration Chart 3. Completes the session in 60 minutes +/- 10 minutes 4. Utilizes the treatment manual script as appropriate (rate on a scale of 0-10) 5. Completes worksheets according to the manual (0-10) 6. Identifies and addresses the main reasons for the individual's difficulties with adherence as it relates to the module (0-10) 7. Allots sufficient time for and appropriately answers questions or describes concepts that are unclear to the participant (0-10) 8. Sets up next follow-up time/visit, provides contact information, and reviews recommended procedures for contacting staff in the event that future appointments need to be rescheduled. • Methods • CAE has been manualized as a series of the following four treatment modules: • Psychoeducation • Patient training in communication with care providers • Training in medication routines • Modified motivational interviewing to address substance abuse References Zaretsky AE, Rizvi S, Parikh SV. How Well Do Psychosocial Interventions Work in Bipolar Disorder?. Can J Psychiatry. 2007;52: 14-19 Taylor CB, Chang VY. Issues in the dissemination of cognitive-behavior therapy. Nord J Psychiatry. 2008;62(suppl 47): 37-44. Vakoch DA, Strupp HH. The evolution of psychotherapy training: reflections on manual-based learning and future alternatives. J Clin Psychology.2000;56(3): 309-318. Bauer MS, McBride L. Manual-based psychotherapy for bipolar disorder: a feasibility study. J Clin Psychiatry. 1998;59: 449-455.