Download
1 / 28
280 likes | 446 Views
The intraorbital part of the optic nerve…. is longer than the distance from the back of the globe to the optic foramen. the roof of the orbit is adjacent to…. frontal sinus anterior cranial fossa. the floor of the orbit is adjacent to…. maxillary sinus. The medial wall of the orbit is….

E N D
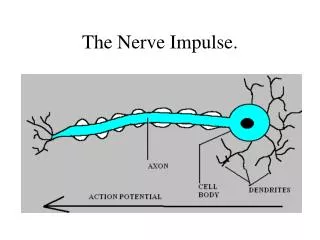
The intraorbital part of the optic nerve… • is longer than the distance from the back of the globe to the optic foramen.
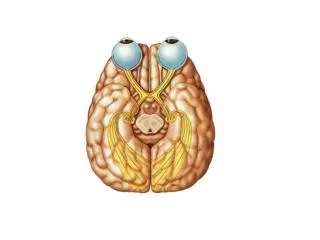
the roof of the orbit is adjacent to… • frontal sinus • anterior cranial fossa
the floor of the orbit is adjacent to… • maxillary sinus
The medial wall of the orbit is… • thin and adjacent to the ethmoid sinus • “lamina paprycia”
what passes through the orbital fissures? • blood • nerves (branches of III, IV, V, VI
name the 9 general signs of orbital disease • soft tissue signs • proptosis • enophthalmos • ophthalmoplegia • dynamic signs • optic disc changes • choroidal folds • retina vascular changes • vision reduction
general causes of orbital disease • thyroid (Graves) disease • infections in & around orbit • inflammation • vascular malformations • space occupying lesions • craniosynostoses
quick review of Grave’s disease • autoimmune • IgG causes EOM enlargement (as well as hyperthyroidism due to IgG “fitting” the TSH receptors in thyroid) • results in increased orbital contents endophthalmos • Signs: • Dalrymple • VonGraefe • Kocher
describe the Dalrymple sign in Graves disease • lid retraction in primary gaze • “Do you see superior sclera on forward gaze?” • Normally the superior lid should rest 2mm below the limbus.
Describe the VonGraefe sign in Graves disease • retarded descent of the upper lid on downward gaze
Describe the Kocher sign in Graves disease • a staring and frightened appearance of the eyes which is particularly marked on attentive fixation
Differentiate between: Preseptal Orbital proptosis ophthalmoplegia (+) APD reduced VAs • no proptosis • FROM of EOM’s • normal pupils • normal VAs
Overview of rhino-orbital mucormycosis • rare opportunistic infection caused by Mucoraceae fungi • typically affects patients with: • diabetic ketoacidosis • compromised immune systems • inhalation of spores upper respiratory infection contiguous sinuses orbit & brain
signs & symptoms of rhino-orbital mucormycosis • symptoms: • gradual-onset facial and periorbital swelling • diplopia • visual loss • signs: • ischemic infarction superimposed on septic necrosis responsible for black eschar which may develop on palate, turbinates, nasal septum, skin and eyelids • ophthalmoplegia • progression is slower than orbital cellulitis
treatment of mucormycosis • IV amphotericin • daily packing & irrigation of involved areas with amphotericin • wide excision of devitalized & necrotic tissues • hyperbaric oxygen may be helpful • correction of underlying metabolic defect • exenteration may be required in severe unresponsive cases
Name the inflammatory orbital diseases • idiopathic • acute dacryoadenitis • orbital myositis • Tolusa-Hunt Syndrome
“new name” for orbital pseudo-tumor • idiopathic orbital inflammatory disease (IOID)
IOID symptoms, signs, treatment • Symptoms • 3rd to 6thdecate • acute readness • swelling • pain • usually unilateral in adults; can be bilateral in children • Signs • congestive proptosis • ophthalmoplegia • optic nerve dysfunction if posterior orbit involved • Treatment • observation for mild cases • oral steroids effective for 50-75% of moderate—severe cases.
IOID differential • bacterial orbital cellulitis • severe acute thyroid eye disease • systemic disorders • Wegener granulomatosis • polyarteritisnodosa • Waldenströmmacroglobulinemia • ruptured dermoid cyst
acute dacryoadenitis symptoms, signs & treatment • Symptoms • acute discomfort in region of lacrimal gland (superior temporal globe) • Signs • swelling of lateral aspect of eyelid ‘S’ shaped ptosis • globe displaced downward & inward • tenderness over lacrimal gland fossa • injection of palpebral portion of lacrimal gland & adjacent conjunctiva • lacrimal secretion may be reduced • Treatment • ~25% occur with IOID • more commonly, occur in isolation & resolve spontaneously • usually does NOT require treatment • Must rule-out infection & space occupying lesion of lacrimal gland.
orbital myositis general points • inflammation of at least one EOM • usually young adult with acute pain worsened by eye movements & diplopia • injection over involved muscle
orbital myositis differential & treatment • differential • orbital cellulitis • thyroid eye disease • Tolosa-Hunt syndrome • Treatment • NSAIDs for mild disease • systemic steroids (although recurrences occur in 50% of cases) • radiotherapy
Tolosa-Hunt syndrome • non-specific granulomatous inflammation of cavernous sinus, superior orbital fissure and/or orbital apex • Symptoms • diplopia associated with ipsilateralperiorbital or hemicranial pain • Signs • proptosis (mild if present) • CN III palsies w/pupil involvement • sensory loss along 1st & 2nd divisions of CN V • Treatment • systemic steroids
describe carotid-cavernous fistula • when carotid arterial blood flows into ophthalmic veins leading to ocular signs because of venous and arterial stasis around eye and orbit • increased episcleral venous pressure • decrease in arterial flow to CN in cavernous sinus
describe anatomy of cavernous sinus • Wall • CN III • CN IV • CN V1 & V2 • Sinus • CN VI • autonomic plexis • internal carotid
classification of carotid-cavernous fistulas • high flow • 70—90% of all CCFs • blood from carotid artery flows directly into cavernous sinus • defect in internal carotid • caused by trauma (most common) or spontaneous rupture • signs: pulsatileproptosis, chemosis, intracranial noise • low flow • blood flows indirectly via meningial branches • more subtle symptoms • greater than normal pulsation on Goldmann measurement
high-flow carotid cavernous fistula ocular signs • ocular bruit reduced with carotid compression against neck • increased IOP • anterior segment ischemia (corneal epithelial edema, cells & flare, iris atrophy, cataract and rubeosisiridis) • ophthalmoplegia • fundus signs: optic disc swelling, venous dilation, intraretinal hemorrhage
low-flow carotid-cavernous fistula ocular signs • gradual, chronic redness due to episcleral venous engorgement • greater than normal pulsation on Goldmanntonometry • milder signs of high-flow CCF