Download
1 / 26
260 likes | 418 Views
TREATMENT OF SMALL VEINS. SENTARA COSMETIC AND LASER TREATMENT CENTER. CHRISTI SILER, R.N. Examples of Small Veins. Etiology of Venous Disease. Heredity- Primary cause Pregnancy Obesity Standing or sitting for long periods of time Trauma Incidence- 80% female & 20% male.

E N D
TREATMENT OF SMALL VEINS SENTARA COSMETIC AND LASER TREATMENT CENTER CHRISTI SILER, R.N.
Etiology of Venous Disease • Heredity- Primary cause • Pregnancy • Obesity • Standing or sitting for long periods of time • Trauma • Incidence- 80% female & 20% male
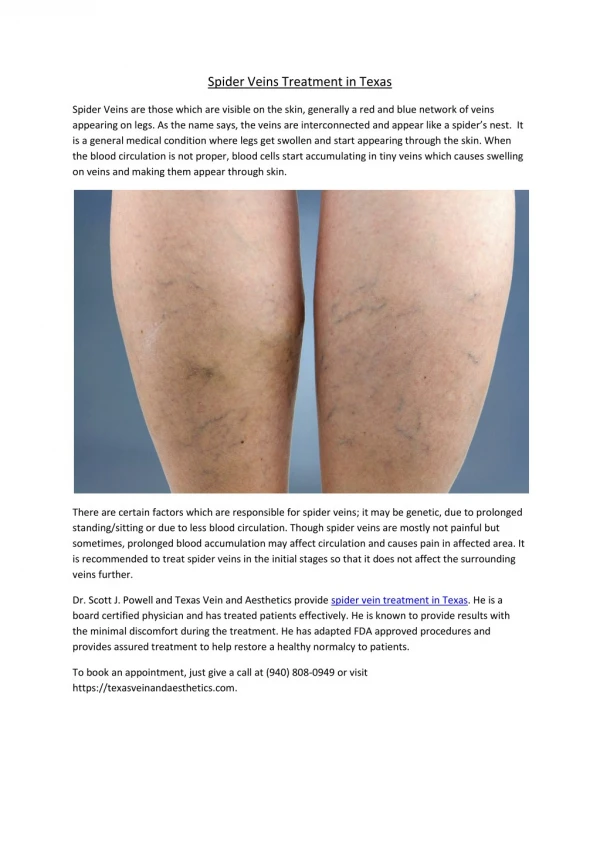
Microanatomy of Venous System Spider Veins Reticular Vein Perforator
Algorithm for Small Vessel Treatment • Rule out truncal insufficiency- plan to correct if present • Determine system involved • Identify associated reticular veins • Perform appropriate treatment • Compression for 5-7 days • Follow-up & re-treat in 4-6 weeks
Lateral Reticular Vein with associated telangiectasia
Small Vein Treatment Options • Sclerotherapy- still the Gold Standard • Lasers- great adjunct to treatment • Non lasers- IPL, Ohmic Thermolysis, Vascutouch • Microphlebectomy- for large reticular veins • Combination Therapy- BEST OPTION for quickest and cosmetically superior results
The IdealSclerosant • Non-allergenic/ Non-toxic • Painless • No risk of hyperpigmentation • No risk of telangiectatic matting • No ulceration • FDA approved • UNFORTUNATELY, no sclerosant meets all of this criteria
Detergent Properties • Efficient sclerosant- causes intimal inflammation thrombus formation fibrous tissue vein obliteration • Painless • Low rate of allergies • Low rate of pigmentation • Extravasation tolerated at low amounts
Reticular Veins • R/O truncal insufficiency/ incompetent perforators • Inject reticular veins first • Follow with laser/ sclerotherapy to telangiectasias • Compression dressing post tx facilitates clotting
Why Combination Therapy? Laser spider veins first Vessel damage d/t heat Decreased intimal lumen Less sclerosant needed Lower incidence of hyperpigmentation TWICE THE DAMAGE MEANS TWICE AS FAST!
Lasers- Not All are Created Equal • 940 nm and 1064 nm most common for treatment of telangiectasias • Goal is to cause vessel damage without damaging surrounding tissue • No sun exposure or sunless tanning prior to tx • Test laser and sclerotherapy at consultation to assess response and candidacy for treatment
Foam Sclerotherapy • CO2 vs. Room Air • CO2 bubbles dissolves faster in arterial circulation, thus reducing the risk of adverse event • Tessari Method- • 1 part solution: 4 parts gas • Stopcock, 2 syringes
Advantages- • Increases surface area of sclerosant, thus reducing amount • of drug needed • Circumferential contact with intimal wall causes more damage/ • better result • Displaces blood, thus avoiding dilution of drug/ increases • efficacy • Disadvantages- • Patients with PFO may not be candidate • Neurological deficits- • Migraine • Scotoma • DVT- clear deep system with foot dorsiflexion immediately • post tx and encourage ambulation
Adverse Sequelae • Post Sclerotherapy Hyperpigmentation- transient • Localized Urticaria d/t inflammatory response/ histamine release • Angiogenesis/ Telangiectatic Matting- R/O truncal insufficiency or perforators to decrease risk • Discomfort at injection site • Recurrence- hereditary
Complications • Cutaneous necrosis • Superficial thrombophlebitis • DVT • Nerve Injury • Allergic Reaction • Migraine • Scotoma
In Summary • Reticular veins & associated telangiectasia can be easily treated in the office setting • R/O truncal insufficiency or incompetent perforators • Microphlebectomy if needed for large reticular veins • Laser/ RF first and follow with sclerotherapy • Foam sclerotherapy to reticular veins if appropriate candidate • Dilute sclerotherapy to telangiectasia • Most patients require 3-5 treatments spaced 4-6 weeks apart for optimal results