Download
1 / 1
10 likes | 107 Views
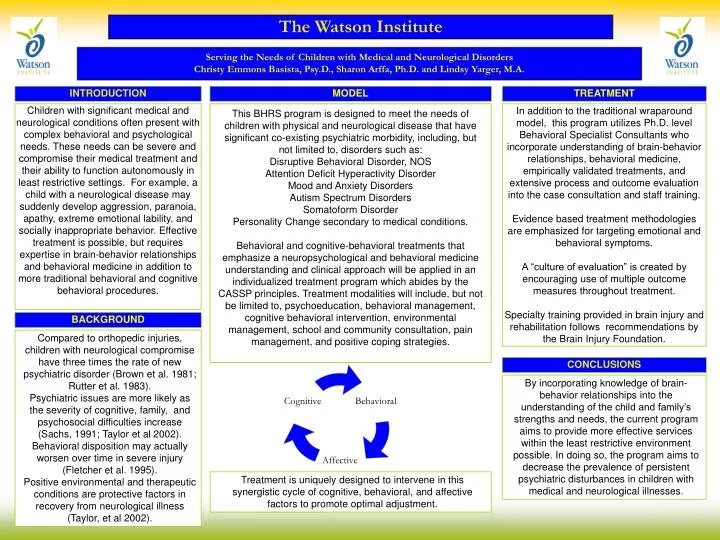
The Watson Institute. Serving the Needs of Children with Medical and Neurological Disorders Christy Emmons Basista, Psy.D., Sharon Arffa, Ph.D. and Lindsy Yarger, M.A. TREATMENT. INTRODUCTION. MODEL.

E N D
The Watson Institute Serving the Needs of Children with Medical and Neurological Disorders Christy Emmons Basista, Psy.D., Sharon Arffa, Ph.D. and Lindsy Yarger, M.A. TREATMENT INTRODUCTION MODEL Children with significant medical and neurological conditions often present with complex behavioral and psychological needs. These needs can be severe and compromise their medical treatment and their ability to function autonomously in least restrictive settings. For example, a child with a neurological disease may suddenly develop aggression, paranoia, apathy, extreme emotional lability, and socially inappropriate behavior. Effective treatment is possible, but requires expertise in brain-behavior relationships and behavioral medicine in addition to more traditional behavioral and cognitive behavioral procedures. This BHRS program is designed to meet the needs of children with physical and neurological disease that have significant co-existing psychiatric morbidity, including, but not limited to, disorders such as: Disruptive Behavioral Disorder, NOS Attention Deficit Hyperactivity Disorder Mood and Anxiety Disorders Autism Spectrum Disorders Somatoform Disorder Personality Change secondary to medical conditions. Behavioral and cognitive-behavioral treatments that emphasize a neuropsychological and behavioral medicine understanding and clinical approach will be applied in an individualized treatment program which abides by the CASSP principles. Treatment modalities will include, but not be limited to, psychoeducation, behavioral management, cognitive behavioral intervention, environmental management, school and community consultation, pain management, and positive coping strategies. In addition to the traditional wraparound model, this program utilizes Ph.D. level Behavioral Specialist Consultants who incorporate understanding of brain-behavior relationships, behavioral medicine, empirically validated treatments, and extensive process and outcome evaluation into the case consultation and staff training. Evidence based treatment methodologies are emphasized for targeting emotional and behavioral symptoms. A “culture of evaluation” is created by encouraging use of multiple outcome measures throughout treatment. Specialty training provided in brain injury and rehabilitation follows recommendations by the Brain Injury Foundation. BACKGROUND • Compared to orthopedic injuries, children with neurological compromise have three times the rate of new psychiatric disorder (Brown et al. 1981; Rutter et al. 1983). • Psychiatric issues are more likely as the severity of cognitive, family, and psychosocial difficulties increase (Sachs, 1991; Taylor et al 2002). • Behavioral disposition may actually worsen over time in severe injury (Fletcher et al. 1995). • Positive environmental and therapeutic conditions are protective factors in recovery from neurological illness (Taylor, et al 2002). CONCLUSIONS • By incorporating knowledge of brain-behavior relationships into the understanding of the child and family’s strengths and needs, the current program aims to provide more effective services within the least restrictive environment possible. In doing so, the program aims to decrease the prevalence of persistent psychiatric disturbances in children with medical and neurological illnesses. • Treatment is uniquely designed to intervene in this synergistic cycle of cognitive, behavioral, and affective factors to promote optimal adjustment.