Download
1 / 1
10 likes | 167 Views
SOCIAL EXCLUSION AND RASHTRIYA SWASTHYA BIMA YOJANA (RSBY - NATIONAL HEALTH INSURANCE SCHEME) IN MAHARASHTRA, INDIA H. Thakur*, S. Ghosh, A. Nawkar School of Health Services Studies, Tata Institute of Social Sciences, India *harshad@tiss.edu. www.healthinc.eu. Key Findings.

E N D
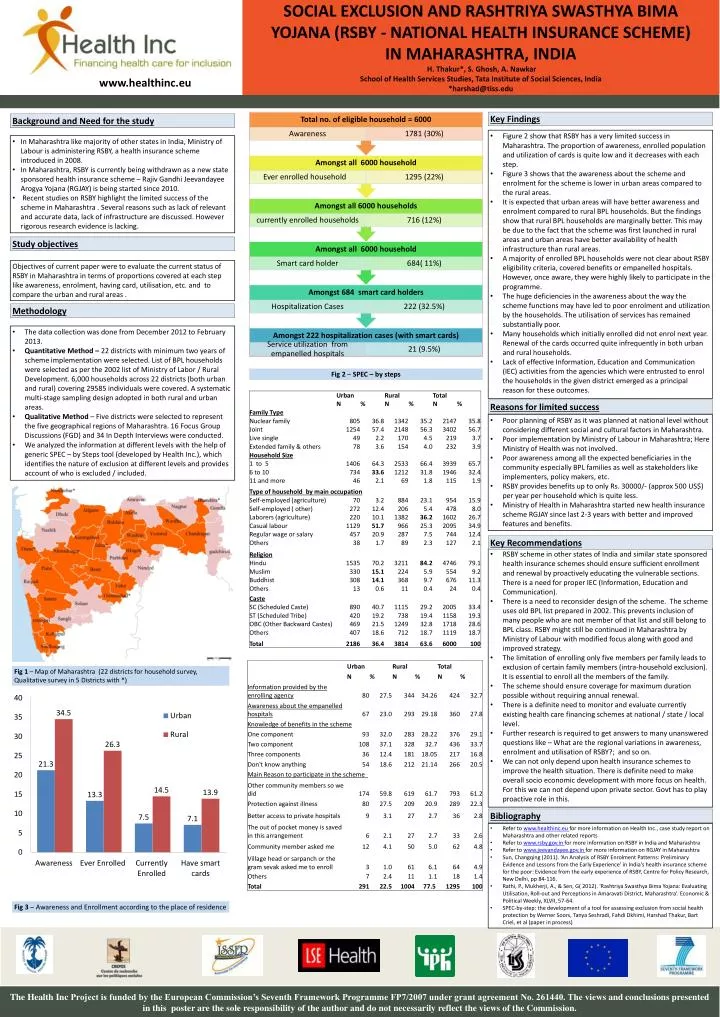
SOCIAL EXCLUSION AND RASHTRIYA SWASTHYA BIMA YOJANA (RSBY - NATIONAL HEALTH INSURANCE SCHEME) IN MAHARASHTRA, INDIA H. Thakur*, S. Ghosh, A. NawkarSchool of Health Services Studies, Tata Institute of Social Sciences, India*harshad@tiss.edu www.healthinc.eu Key Findings Background and Need for the study • Figure 2 show that RSBY has a very limited success in Maharashtra. The proportion of awareness, enrolled population and utilization of cards is quite low and it decreases with each step. • Figure 3 shows that the awareness about the scheme and enrolment for the scheme is lower in urban areas compared to the rural areas. • It is expected that urban areas will have better awareness and enrolment compared to rural BPL households. But the findings show that rural BPL households are marginally better. This may be due to the fact that the scheme was first launched in rural areas and urban areas have better availability of health infrastructure than rural areas. • A majority of enrolled BPL households were not clear about RSBY eligibility criteria, covered benefits or empanelled hospitals. However, once aware, they were highly likely to participate in the programme. • The huge deficiencies in the awareness about the way the scheme functions may have led to poor enrolment and utilization by the households. The utilisation of services has remained substantially poor. • Many households which initially enrolled did not enrol next year. Renewal of the cards occurred quite infrequently in both urban and rural households. • Lack of effective Information, Education and Communication (IEC) activities from the agencies which were entrusted to enrol the households in the given district emerged as a principal reason for these outcomes. • In Maharashtra like majority of other states in India, Ministry of Labour is administering RSBY, a health insurance scheme introduced in 2008. • In Maharashtra, RSBY is currently being withdrawn as a new state sponsored health insurance scheme – Rajiv Gandhi Jeevandayee Arogya Yojana (RGJAY) is being started since 2010. • Recent studies on RSBY highlight the limited success of the scheme in Maharashtra . Several reasons such as lack of relevant and accurate data, lack of infrastructure are discussed. However rigorous research evidence is lacking. Study objectives Objectives of current paper were to evaluate the current status of RSBY in Maharashtra in terms of proportions covered at each step like awareness, enrolment, having card, utilisation, etc. and to compare the urban and rural areas . Methodology • The data collection was done from December 2012 to February 2013. • Quantitative Method – 22 districts with minimum two years of scheme implementation were selected. List of BPL households were selected as per the 2002 list of Ministry of Labor / Rural Development. 6,000 households across 22 districts (both urban and rural) covering 29585 individuals were covered. A systematic multi-stage sampling design adopted in both rural and urban areas. • Qualitative Method – Five districts were selected to represent the five geographical regions of Maharashtra. 16 Focus Group Discussions (FGD) and 34 In Depth Interviews were conducted. • We analyzed the information at different levels with the help of generic SPEC – by Steps tool (developed by Health Inc.), which identifies the nature of exclusion at different levels and provides account of who is excluded / included. Fig 2 – SPEC – by steps Reasons for limited success • Poor planning of RSBY as it was planned at national level without considering different social and cultural factors in Maharashtra. • Poor implementation by Ministry of Labour in Maharashtra; Here Ministry of Health was not involved. • Poor awareness among all the expected beneficiaries in the community especially BPL families as well as stakeholders like implementers, policy makers, etc. • RSBY provides benefits up to only Rs. 30000/- (approx 500 US$) per year per household which is quite less. • Ministry of Health in Maharashtra started new health insurance scheme RGJAY since last 2-3 years with better and improved features and benefits. Key Recommendations • RSBY scheme in other states of India and similar state sponsored health insurance schemes should ensure sufficient enrollment and renewal by proactively educating the vulnerable sections. There is a need for proper IEC (Information, Education and Communication). • There is a need to reconsider design of the scheme. The scheme uses old BPL list prepared in 2002. This prevents inclusion of many people who are not member of that list and still belong to BPL class. RSBY might still be continued in Maharashtra by Ministry of Labour with modified focus along with good and improved strategy. • The limitation of enrolling only five members per family leads to exclusion of certain family members (intra-household exclusion). It is essential to enroll all the members of the family. • The scheme should ensure coverage for maximum duration possible without requiring annual renewal. • There is a definite need to monitor and evaluate currently existing health care financing schemes at national / state / local level. • Further research is required to get answers to many unanswered questions like – What are the regional variations in awareness, enrolment and utilisation of RSBY?; and so on. • We can not only depend upon health insurance schemes to improve the health situation. There is definite need to make overall socio economic development with more focus on health. For this we can not depend upon private sector. Govt has to play proactive role in this. Fig 1 – Map of Maharashtra (22 districts for household survey, Qualitative survey in 5 Districts with *) Bibliography • Refer to www.healthinc.eufor more information on Health Inc., case study report on Maharashtra and other related reports • Refer to www.rsby.gov.infor more information on RSBY in India and Maharashtra • Refer to www.jeevandayee.gov.infor more information on RGJAY in Maharashtra • Sun, Changqing (2011). ‘An Analysis of RSBY Enrolment Patterns: Preliminary Evidence and Lessons from the Early Experience’ in India’s health insurance scheme for the poor: Evidence from the early experience of RSBY, Centre for Policy Research, New Delhi, pp 84-116. • Rathi, P., Mukherji, A., & Sen, G( 2012). ‘Rashtriya Swasthya Bima Yojana: Evaluating Utilisation, Roll-out and Perceptions in Amaravati District, Maharashtra’. Economic & Political Weekly, XLVII, 57-64. • SPEC-by-step: the development of a tool for assessing exclusion from social health protection by Werner Soors, Tanya Seshradi, FahdiDkhimi, Harshad Thakur, Bart Criel, et al (paper in process) Fig 3 – Awareness and Enrollment according to the place of residence The Health Inc Project is funded by the European Commission’s Seventh Framework Programme FP7/2007 under grant agreement No. 261440. The views and conclusions presented in this poster are the sole responsibility of the author and do not necessarily reflect the views of the Commission.
