Download
1 / 17
170 likes | 298 Views
Pediatricians’ Obligations to Care for Under- and Uninsured Children. Joel Frader, MD, MA A Todd Davis Professor of General Academic Pediatrics and Professor of Medical Humanities and Bioethics Children’s Memorial Hospital and Feinberg School of Medicine, Northwestern University Chicago, IL.

E N D
Pediatricians’ Obligations to Care for Under- and Uninsured Children Joel Frader, MD, MA A Todd Davis Professor of General Academic Pediatrics and Professor of Medical Humanities and Bioethics Children’s Memorial Hospital and Feinberg School of Medicine, Northwestern University Chicago, IL
Overview • Two ethical bases for providing “free” care • Physicians have considerable economic privilege acquired in part through social resources • Privilege creates moral obligations to disadvantaged • Physicians as professionals have duty to share specialized knowledge and skills • Nevertheless, extent of obligation unclear
Physicians’ Socioeconomic Status: Substantial Privilege • Bureau of Labor Statistic 2009 data indicate • Median income general pediatricians $161,410 • Geographic variation • Vermont: $116K • Minnesota: $199K • Iowa: $206K • Census Bureau 2009 data indicate • U.S. median household income $50, 221
More Income Data In 2008, those earning > $159,600 in top 5% of earners In 2006, top 6.4% of earners accounted for 1/3 of all income in U.S. Political economists define top 5% of earners as “rich,” top 1% as “upper class” Scholars’ definitions do not = how people feel
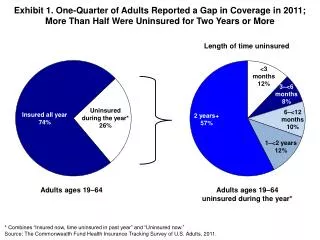
Insured/Not Insured Children • AAP data (Feb. 2010 AAP Fact Sheet) • In 2008 • ~60% children with private health insurance • ~30% children covered by Medicaid, CHIP • ~10% children with no coverage • AAP 2000 membership survey (all responders) • 67% AAP members said they accept all Medicaid patients • Regional variation: 48% Oklahoma to 94% Mass.
Pediatricians’ Reasons for Restricting or Refusing Medicaid Patients Low reimbursement rates Burdensome paperwork 1/3 of survey respondents indicated they would ↑ number of Medicaid patients if reimbursement ↑ 54% said Medicaid did not cover overhead 35% did not know if Medicaid covered overhead
AAP 2000 Survey: Private Office-Based Practitioners’ Responses • 55% accept all Medicaid/SCHIP patients • 52% if said caseload at capacity • 59% if said caseload under capacity • Of those limiting Medicaid pts., respondents indicated payment would need to rise to 83% of usual fee to accept more Medicaid pts. and 87% of usual fee to accept all Medicaid pts.
Conclusions from Facts Most general pediatricians earn in top 5% of U.S. incomes 40% of children in U.S. have Medicaid or no health insurance 33% of U.S. pediatricians, on average, limit number of patients with Medicaid Reimbursement rates and paperwork burden account for Medicaid refusals
Nature of Professional Obligations Despite high charges, tuition does not cover cost of educating medical students Portion of cost from scholarships (philanthropy) and institutional grant overhead, etc. Costs of post-graduate education also, in part, from Medicare GME payments to teaching hospitals and programs for childrens’ hospitals Socialized cost of medical education provides knowledge/skills permitting later relative wealth
Meaning of Being a Professional • Professionals have • Grant from society to practice based on specialized knowledge and skills • Monopoly on (most) aspects of practice, including fees • General freedom from state control of practice • These entail substantial social power • Above creates responsibilities to provide service to those who can benefit from professionals’ skills, even if professional inconvenienced or at risk • Need for service independent of ability to pay
An Important Aside • This talk concerns pediatricians • The arguments about • Relative wealth • Socialized costs of professional education • Duties of professionals to use knowledge/skills to benefit even those who cannot pay • Apply equally to lawyers, MBAs, accountants, dentists, etc. Not picking on us
From Howard Brody, MD, PhD “[A physician’s] privileged economic status raises difficult questions about the ability of the physician to attend to the patient’s interest and to serve as an effective advocate for the patient when additional services may be helpful. And it creates a power disparity between physician and patient that may be hard to bridge.” The Healer’s Power, 1992
From Paul Menzel, PhD “The argument should not so much focus on the particular question of whether two, three, or five times the average worker’s earnings is the proper income level for doctors….It is utterly hypocritical for doctors…to close their eyes to the level of doctors’ incomes amidst otherwise vigorous concern for making health care worth the increasing money we pay for it.” Or concern for access to care…Medical Costs, Moral Choices, 1983
The Crux of the Matter Physicians, including general pediatricians, in the U.S. enjoy economic privilege Many children in the U.S. have reduced access to pediatricians because they lack private insurance Pediatricians have a duty to repay society for subsidizing their education Pediatricians have a professional (moral) duty to use their special knowledge to benefit members of society who cannot pay the usual fees
But How Much? Pediatricians deserve to make a decent income Is a decent income 3X, 4X, 5X the median? Many religious traditions suggest that one should contribute 10-20% of one’s income to some good cause (one’s church, charity, etc.) We will never agree on the extent to which those with privilege should give to those without
Nevertheless… • Few acceptable arguments for refusing to care for any Medicaid or uninsured patients • If the 1/3 of U.S. pediatricians who now refuse to accept patients with Medicaid and/or the uninsured began to provide care for some of these patients it would: • Increase access to care for many who have none • Spread the economic burden among pediatricians more evenly, perhaps permitting care for additional patients lacking private insurance
Conclusion • Viewing the practice of pediatrics simply as a matter of running a business ignores: • The moral nature of professional practice (service) • The universal need for access to medical care • The socially subsidized nature of medical education and residency training • The economic privilege of physicians and the social and moral tensions that privilege creates