Download
1 / 58
580 likes | 1.01k Views
Clinical Otology. Balasubramanian Thiagarajan. Symtoms. Deafness Discharge Tinnitus Pain Vertigo. Deafness. Onset. Gradual. Sudden. Trigger. Sudden hearing loss (SN). Loss of atleast 30 dB in atleast three contiguous frequencies over a period of less than 3 days. Viral causes

E N D
Clinical Otology Balasubramanian Thiagarajan
Symtoms • Deafness • Discharge • Tinnitus • Pain • Vertigo
Deafness Onset Gradual Sudden Trigger
Sudden hearing loss (SN) • Loss of atleast 30 dB in atleast three contiguous frequencies over a period of less than 3 days. • Viral causes • Vascular causes • Hearing loss is the only symptom • High dose prednisolone may be useful
Sensorineural hearing loss (Sudden) • Transverse fracture of pertrous bone • Auto immune reaction following trauma / infection • Inflammatory reaction (Viral infections) • Vascular compromise
Conductive hearing loss - (Sudden) • Ossicular disruption • Haemotympanum (transient) • Failed attempts to remove cerumen
Mixed hearing loss - (Sudden) • Fractures involving petrous bone • Auto immune reaction to proteins released due to traumatic injury
Gradual progressive hearing loss • Inflammatory • Degenerative
Fluctuating hearing loss • Impacted cerumen • Meniere's disease • Perilymph fistula
Differentiating Conductive / SN loss • Difficulty in comprehending spoken words • Deafness associated with tinnitus • Intolerance to loud sounds • Tuning fork tests
Discharge • Quantity • Quality • Duration of discharge • Aggravating / releiving factors
Ear discharge - quality • Mucoid - CSOM • Mucopurulent - CSOM with mastoiditis • Serous - ASOM • Serosanguinous - ASOM, Otitis externa, trauma • Watery - CSF otorrhoea
Ear discharge - causes • ASOM • CSOM • Otomycosis • CSF otorrhoea
Tinnitus • Wax • Active otosclerosis • Sensorineural hearing loss • Ototoxic drugs • Objective tinnitus - Patulous ET, Palatal myoclonus
Pain • Otalgia • Referred otalgia
Ear pain 5,6,10th cranial nerves C2 & C3 Tragal tenderness + impated wax Referred otalgia Tragal tenderness - Tragal tenderness + Otalgia Otomcosis Myringitis granulosa Tragal tenderness + Tragal tenderness - AOM Keratosis obturans Tragal tenderness + Furuncle
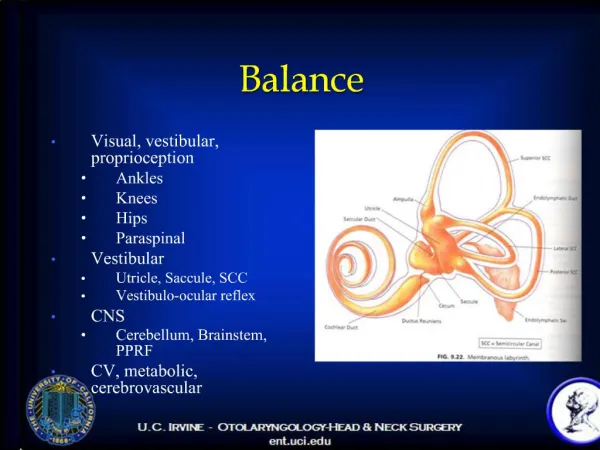
Vertigo • Sensation of unsteadiness / rotation • Diseases if inner ear cause vertigo • Associated with tinnitus and hard of hearing • Peripheral vertigo
Nystagmus • Spontaneous / evoked • Direction of nystagmus - Right beating, left beating, geotrophic, ageotrophic. • Plane - Horizontal, rotatory or vertical • Intensity - (I, II and III degree)
Spontaneous nystagmus • Eye movements without congnitive, visual, vestibular stimulus • Commonly induced by vestibular imbalance • Vestibular nystagmus is typically inhibited by visual fixation • It follows Alexander's law (nystagmus is greater in the direction of fast phases)
Alexander's nystagmus grading • I degree - Present only during gaze in the direction of fast phase • II degree - Present during straight gaze and also increases in the direction of fast phase • III degree - Present during all fields of gaze, but greatest in the direction of fast phase
History should include • Previous ear surgery • Previous head injury • Systemic diseases like diabetes / Hypertension • Use of ototoxic drugs • Noise exposure • Family h/o deafness • H/o atopy / allergy
Inspection of external ear • Shape and size of pinna • Presence of tags, preauricular sinus and pits • Evidence of trauma to pinna • Skin condition over pinna and external canal • Presence of operative scar in post aural area and end aural region • Neoplastic lesions of pinna • Discharge from external canal
Drug history / Occupation • Drugs like gentamycin, Streptomycin, and Aspirin can cause extensive damage to hair cells of cochlea • Noise exposure can cause damage to outer hair cells of cochlea • May be reversible during early phases
Drug induced ototoxicity - Features • Bilateral sensorineural hearing loss • Bilaterally symmetrical hearing loss • Onset time - ??? • Can occur even after a single large dose • Vestibular injury - common (aminoglycosides) • Positional nystagmus - a feature of vestibular injury
Aminoglycosides • Cleared more slowly from inner ear fluids than serum • There exists a latency - deafness may occur even 2 months after cessation of the treatment • Pts on potentially ototoxic aminoglycoside medications should be monitored atleast for a period of 6 months following cessation of the offending drug.
Discharge • Duration • Quantity • Quality • Aggravating & releiving factors
Acute ear discharge - Causes • ASOM - Blood tinged • Otomycosis - Itchy ear, fungal mass seen • CSF otorrhoea
Profuse ear discharge - Causes • Chronic mastoiditis - Mastoid tenderness + May lead to formation of subperiosteal abscess • Mastoid reservoir - Mastoid tenderness on deep palpation + • Extradural abscess
Quality of ear discharge • Mucoid - CSOM • Mucopurulent - CSOM with mastoiditis • Serous - asom • Serosanguinous - ASOM, Otitis externa • Watery - CSF
Tinnitus • Subjective - perceived by the patient • Objective - perceived by both the pt and examiner
Otalgia • Pain in the ear • Could be due to inflammatory pathology affecting the ear • Referred otalgia due to pathology elsewhere
Three finger test • Index, middle and thumb are used. • Index finger is applied over mastoid process - tenderness indicates mastoiditis • Middle finger is applied over well of the concha - tenderness indicates inflammation in the mastoid antrum area • Thumb is used to apply pressure over mastoid process. Tenderness indicates mastoid emissary vein thrombophlebitis
Peripheral vertigo • Is defined as sensation of unsteadiness / rotation • Commonly caused by inner ear disorders • Associated with tinnitus / ear block
Peripheral vertigo - Features • It is fatigable • It is positional • Horizontal nystagmus • Cerebellar signs absent
External ear • Shape / size of pinna • Tags / sinuses / pits • Evidence of trauma to pinna • Perichonditis • Seroma • Skin of pinna / external canal • Discharge from external canal • Evidence of previous surgery • Neoplasm
External canal - Straightening • Aural speculum • Adults - Pinna is pulled postero superiorly • Infants - pinna is pulled posteriorly and downwards
Ear drum • Oval / pearly white in color • Pars tensa • Attic • Cone of light • Handle / lateral process of malleus • Perforations
Cone of light • Present in the antero inferior quadrant • Cone shaped • Caused due to orientation of middle fibrous layer • Broken up in retracted ear drums • Broken up / lost when ear drum bulges
Color of ear drum • Pearly white - normal • Red drum - Glomus jugulare, AOM • Blue drum - SOM, Hemotympanum • Pink drum - Flamingo sign • Chalky drum - Tympanosclerosis
Retraction pocket features • Prominent anterior and posterior malleolar folds • Apparent foreshortening of handle of malleus • Prominent lateral process of incus • Decreased / absent mobility of ear drum • Presence of pockets of retraction
Siegel's speculum • Convex lens • Magnifies 2.5 times • Mobility of ear drum • To suck out secretions from middle ear • To apply ear drops by displacement method
Tuning fork tests • Three frequencies are used • 256Hz, 512 Hz, 1024 Hz • These frequencies fall within speech range • Rinne, Weber and ABC
Prerequisites of a good tuning fork • It should be made of good alloy • Should vibrate for one full minute • Should not produce overtones
Rinne test • All three frequencies can be used • + Rinne (Air conduction better than bone conduction) • -ve Rinne (Bone conduction better than air conduction) • False positive Rinne (occurs in unilateral total hearing loss due to opposite ear hearing)