Download

1 / 96
960 likes | 1.52k Views
JAVED'S PRESENTETION ON PARKINSON'S DISEASE. WELCOME. PARKINSON'S DISEASE.

E N D
JAVED'S PRESENTETION ON PARKINSON'S DISEASE WELCOME
PARKINSON'S DISEASE PRESENTED BY… M0HD JAVED QUERAISHI STUDENT PHYSIOTHERAPIST Pt.J.N.M.MEDICAL COLLEGE,RAIPUR (C.G.) PARALYSIS AGITANS SHAKING PALSY
DEFINATION Marsden in 1994 has defined Parkinson’s Disease as -“ A clinical syndrome dominated by a disorder of movement consisting of Tremor at rest , Rigidity , elements of Bradykinesia ( Slowness of movement ), Hypokinesia ( reduced movement ) , Akinesia (loss of movement) & Postural abnormalities associated with a distinctive pathology consisting of degeneration of pigmented brain stem nuclei , including the Dopaminergic Substantia Nigra Pars compacta (SNPc) with the presence of Lewy bodies in the remaining nerve cells .
( Adapted from Fahn S & Jankovic J in 1992) (1) Primary or Idiopathic Parkinsonism (2) Secondary or Acuired or Symptomatic Pakinsonism(3) Parkinsonism plus syndrome or Parkinsonian syndrome. CLASSIFICATION
PRIMARY OR IDIOPATHIC PARKINSONISM It is a Progressive, Disabling, Primary Neurodegenerative disorder. There are four cardinal signs:-( A ) Tremor( B ) Rigidity( C ) Bradykinesia( D ) Postural instability(A B C are together called as Classical Triad)
It is the collective term for a group of conditions that includes PD as well as several other degenerative brain disorders. The signs & symptoms includes the four cardinal signs of PD. Parkinsonism results from a variety of causes that include infections,toxins,drugs,vascular leisons, tumors & trauma.(Neuroleptic Drugs are considered to be the commonest cause of Secondary Parkinsonism today.) SECONDARY OR SYMPTOMATIC OR ACQUIRED PARKINSONISM
It constitute of heterogenous group of multifaceted disorders characterised by Parkinsonian features, with various combinations of Pyramidal , Cerebellar & Autonomic dysfunctions.( The most common form of Parkinsonism seen by Neurologists today is the Idiopathic variety of Parkinson’s disease) PARKINSONISM PLUS SYNDROME OR PARKINSONIAN SYNDROME
HISTORY (1) In 1817 , James Parkinson first described the PD. His description of the disorder was as follws :-“ Involuntary tremulous motion , with lessened muscular power, in parts not in action & even when supported , with a propensity to bend the trunk forward, & to pass from a walking to a running paces ; the senses & intellects being uninjured.” (2) In 1867, Trousseau noted the muscular rigidity & cog wheeling appearance.
(3)In 1877, Charcot named first disease as Parkinson’s Disease & he noted the absence of facial expression (Masked Facies) as a feature of disorder.(4) In 1880, Charcot listed PD as the 5th most common disease.(5) In 1888, Gower noted that , the malady usually commences after 40 yrs of age.(6) In 1898, Purves Stewart , recognised dystonic posturing of the feet , usually provoked by exercise but occasionally relieved by walking & which could be the first symptom of malady.
(7)In 1913 , Lewy first described the concentric hyaline cytoplasmic inclusion &called it as LEWY BODY.It is observed in the nucleus of Substantia Innominata.(8) In 1919, Tretiakoff was the first to observe the characteristic leisons of Substantia Nigra ie. Depletion of pigmented cells.(9) In 1937, Hassler described the anatomy of Substantia Nigra & in 1938 noticed pathological process of PD for the ventrolateral Pars compacta cell group.
(11) In 1960 , Ehringer & Hornykiewicz demonstrated that in PD Dopamine was markedly reduced in the Substantia Nigra , Caudate nucleus & Putamen.(12) In 1967 , Cotzias shows the clinical benefits of high doses of Levo-Dopa in chronic patient with PD. (10) In 1957, Carlsson showed that cerebral Dopamine was concentrated in thestriatum.
EPIDEMIOLOGY (1) PD occurs in about 1% of the population older than 55 yrs of age.(2) Males are slightly more at risk for developing PD than females.(3) In 10 % cases PD occurs before the age of 40 yrs.(4) Mainly found in Western countries.
CLINICAL FEATURES .(A) It consists of regular , rhythmic , alternate contraction antagonist & agonist muscles @ 4-6 times / second.(B)The tremors occurs due to uninhibited activity of the basal ganglia-cortico-thalamus circuit as a result of degeneration of the striatonigral pathway.(C) It is a rhythmic involuntary movement normally affecting the limbs.(D) It is the 1st complain of the patient but in some patient Bradykinesia is usually the first recognised symptom. (E) Resting tremor present mainly PIN / PILL rolling type as like pin / pill rolls between the thumb & index fingure. (1) TREMORS :-
(F) Frequency is 4-6 times / second in early stage & 6-8 times/ second in later stage.( G ) Maximal at periphery & affects the arm more frequently than the leg.(H) Tremor is increased by stress & disappeared during sleep & goal directed movements. ( I ) The hand which is most affected assumes a posture of flexion of the MCP joints with extension of the more distal joints.
(A) Rigidity is defined as resistance to passive motion that is not velocity dependent.(B) It is manifested as cocontraction of agonist & antagonist muscles due an increase in the supraspinal influences on the normal spinal system causing increase tone in the agonist & the antagonist.There is an increased discharge of gamma motor neurons.(C) The patient usually complains of rigidity as a sensation of heaviness or stiffness of the limbs.(D) Present in almost all cases of PD.(E) Cog wheel type rigidity is present. There is intermittent resistance throughout ROM.Lead pipe rigidity is also seen in some cases. There is constant resistance throughout ROM. (2) RIGIDITY :-
(F) It affects proximal muscles first, mainly shoulders & neck and then progresse to face & extremities and then the whole body.(G) As the disease progresses ; Rigidity becomes more severe.(H) Rigidity decreases the ability of patients to move easily. For eg; loss of bed mobility , loss of reciprocal arm swing during gait.(I) Mental concentration & Emotional tension may increase the amount of rigidity present.(J) Prolonged rigidity results in decreased available ROM & serious secondary complications of contracture & postural deformity.(K) Rigidity also has a direct impact on increasing Resting Energy Expenditure (REE) & fatigue levels.
(A) Bradykinesia refers to slowness & difficulty in maintaining movements.It is theoretically presumed that it could be because of difficulty to the basal ganglia to integrate sensory information.(B) Movements are typically reduced in speed,range & amplitude ; termed hypokinesia.(C) Pateint with PD typically demonstrate micrographia ; an abnormally small hand writing that is difficult to read.(D) Pateint feels difficulties in ADL such as bathing,dressing, rising from a chair,turning over in bed,loss of dexterity & making buttoning etc.(E) Pateint experiences difficulty in integrating two motor programmes at the same time(F) Pateint feels hesitation on initiation of movements & early fatigue. (3) BRADYKINESIA :-
(A) Simians posture or Stooped posture.(B) Head protuted forward , flexion at neck , trunk , elbow , hip & knee.(C) Tandem stance :- walking on a single line with narrow BOS.(D) Balance is poor & patient fall if encounters even minor postural perturbation ( a slight push ) due to loss of postural reflexes. (4) POSTURAL INSTABILITY :-
(5) GAIT :- (A) Parkinsonian gait / Freezing / Festinating / Shuffling / Toe –heel / Hurrying gait.(B) Pateint takes small steps on walking.(C) Pt. feels difficulty in initiating movement & to stop walking once started .(D) There is loss of normal heel toe progression . The toe strikes first.(E) The forward leaning of the trunk moves the body’s COG forward , thus causing the patient to hasten his/her pace in order to catch up COG.(F) Loss of arm swing & pelvic rotation.(G) Stride length decreases & speed increased therefore called as festinating gait.
(H) Stance phase & double support time are lengthened while the period of single limb support is shortened.(I) Pt. are able to stop only when they come in contact with an object or a wall.(J) Turning or changing direction is particularly difficult.
INDIRECT IMPAIREMENTS & COMPLICATIONS (A) Lack of facial expression.(B) Subsequent loss of blinking.(C) Smiling may be possible only on command or volitional effort.(D) This can have a significant impact on social interaction & social disability. (1) MASKED FACE :-
(A) Rotational movement are reduced, resulting in movements that are basically uniplanar (in one plane of of motion ) eg; flexion–extension in saggital plane.(B) There is an overall decrease in total number of movements. (C) Movement impoverishment can lead to mental fatigue & loss of motivation. (2)POVERTY OF MOVEMENT
(A) In a patient of PD fatigue is one of the symptom.(B) The pt. has difficulty in sustaining activity & experiences increasing weakness.(C) Repetitive motor acts may start out strong but decrease in strength as the activity progresses.(D) The 1st few words spoken may be loud & strong but diminish rapidly as speech progresses. (3) FATIGUE:-
(A) Pt. Shows the effects of generalized musculoskeletal deconditioning.(B) The more chronic & generalised the disease becomes , the greater the level of muscle weakness & fatigue.(C) Loss of flexibility.(D) Lack of movement in any body segement leads to contracture development of both contractile & noncontractile tissue.(E) Contarctures mainly developes in hip & knee flexors,hip rotators & adductors, plantarflexors, dorsal spine & neck flexors, shoulders adductors & internal rotators, and elbow flexors.(F) Kyphosis is the most common postural deformity. (4) MUSCULOSKELETAL CHANGES
(G) Some pt. may develop Scoliosis from leanning consistently to one side when sitting or walking.(H) Scoliosis generally results from unequal distribution of rigidity in the trunk.(I) Older pt. with reduced activity levels & poor diet are likely to develop osteoporosis.
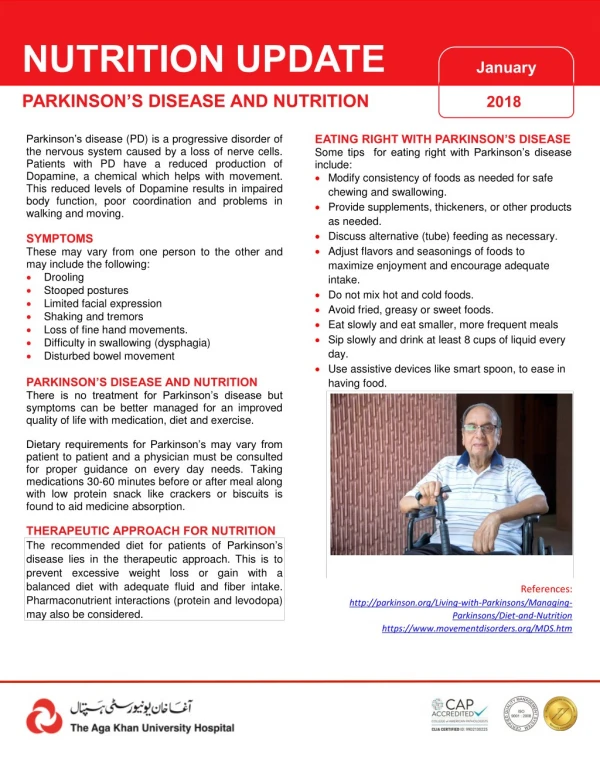
(A) Dysphagia ,impaired swallowing, is present in 50-90 % of pt.(B) Dysphagia can lead to choking or aspiration pnuemonia & impaired nutrition.(C) Dysphagia is the result of rigidity,reduced mobility& restricted range of movement.(D) Pt. experiences problems in all four stages of swallowing;- oral preparatory, oral,pharyngeal & esophageal.(E) Pt. typically experiences excessive drooling (sialorrhea) as a result of increased salivary production & decreased spontaneous swallowing. (5) SWALLOWING DYSFUNCTION:-
(A) Speech is impaired in in 50- 73 % of pt. (B) Hypokinetic Dysarthria; which is characterised by decreased volume , monotone or monopitch speech, imprecise or distorted disarticulation& uncontrolled speech rate. (C) Speech difficulties are also result of rigidity & bradykinesia.(D) Patients experiences reduced mobility , restricted range of movement& uncontrolled rate of movement of muscles controlling respiration , phonation , resonation & articulation. (6) COMMUNICATION DYSFUNCTION:-
(A) Visual disturbances are common in PD. These can include blurring of vision & difficulty in reading which is not coeected by glasses .(B) Conjugate gaze & saccadic eye movements may also be impaired.(C) Eye movements may have a jerky & cog wheeling quality.(D) Pupillary abnormalities are also possible with decreased reflex responses to light & nocciceptive stimuli.(E) 50% patient experiences paresthesias & pain.This can include sensations of numbness ,tingling, abnormal temperature & pain that is cramp like & poorly localized.(F) Postural stress syndrome.(G) Akathisia; it is often described as painful and interferes with relaxation & sleep (7) VISUAL & SENSORYMOTOR DISTURBANCES :-
(A) Dementia occurs in approximately 1/3rd of the patients with PD.(B) Bradyphrenia, a disorder of intellectual function, is common in pt. It is characterised by a slowing of thaught processes with lack of cocentration & attention. (C) Pt. May also demonstrate learning deficits.(D) Perceptual deficits also present.(E) Deficits have been reported in vertical perception, topographic orientation, body shceme and spatial relations. (8) COGNITIVE DYSFUNCTION:-
(A) Depression is the most common,occuring in25-40% of pt.(B) Pt. may demonstrate symptoms of major depression ,including apathy, passivity,loss of ambition or enthusiasm & changes in appetite,sleep and dependency. Suicidal thaughts may be present.(C) Dysthymic disorder characterised by variability in dysphoric mood, or typical depression characterised by intermittent episodes of severe anxiety.(D) Drug related psychoses can occur. (9) BEHAVIOURAL DYSFUNCTION:-
(A)Dysautonomia ; autonomic nervous system dysfunction occurs in pt.(B) Commons problems includes excessive perspiration,greasy skin,increased salivation,thermoregulatory abnormalities(including uncomfertable sensations of heat or cold).(C) Bladder dysfunction includes urinary frequecy, urgency & nocturia.(D)Sexual dysfunction includes impotence.(E) Patient have low appetites & decreased motility of the GIT.(F) Constipation is also problem seen in pt. (10) AUTONOMIC DYSFUNCTION :-
(A) Pulmonary function impairement is reported in 84% of pateints.(B) Orthostatic hypotension & low resting blood presure.Cardiac arrhythmias can also occurs as aresult of L-Dopa .(C) Airway obstruction leads to pulmonary failure.(D) Bradykinetic disorganisation of of respiratory movements.(E)Restrictive dysfunction due to decreased chest expansion that occurs as a result of rigidity of trunk muscles , loss of musculoskeletal flexibility & kyphotic posture. (11) CARDIOPULMONARY DYSFUNCTION:-
(F) Decrease in FVC , FEV1 & increase in RV , RAW (airway resistance).(G) In long standing disease, the lower extremities may exhibit circulatory changes owing to venous pooling as a result of decreased mobility & prolonged sitting. Thus pt. can present with mild to moderate edema of the feet & ankles , which usually subsides during sleep.
(A)Dermatitis can occur due to increased secretion by sweat & sebaceous glands. (12) SKIN INFECTIONS :-
(A) Tapping forehead causes repititive blinking. (13) GLABELLAR TAP SIGN :-
(A) It is present in 75 – 90 % of pt. (14) OALFACTORY DYSFUNCTION :-
ARE YOU SLEEPING.......? DON'T DARE TO SLEEP
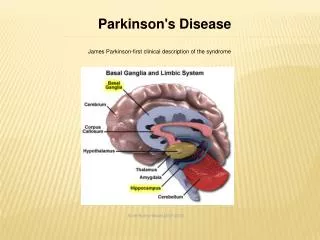
DEFINITION :-The term Basal Ganglia is applied to group of nuclei (mass of gray matter) in the fore brain & upper part of the brain stem that have motor function of great importance . It is the primary motor area in lower animals ( reptiles & birds). BASAL NUCLEI OR BASAL GANGLIA (BG)
The BG includes :-(1) Caudate nucleus – it possesses a head and a tail.(2) Putamen – a Latin word for shell.(3) Globus pallidus or Pallidium or Paleostriatum- it is subdivided into external & internal segment.(4) Subthalamic nucleus (BODY OF LUYS) – it is located in the diencephalon ventral to the thalamus & lateral to the hypothalamus.(5) Substantia nigra – it has two parts ; (a) dorsomedial part is Pars compacta (b) ventrolateral part is Pars reticulata.(Substantia Nigra Pars compacta{SNPc} contains Dopaminergic neurons which produces the Dopamine. Dopamine has inhibitory action.
The scheme of subdivisions of the BG components is shown as follows :-(1) Putamen + Caudate nucleus = Neostriatum or striatum.(2) Putamen + Globus pallidus = Lentiform nucleus.(3) Lentiform nucleus + Caudate nucleus = Corpus striatum.
(A)The corpus striatum has a rich concentration of Acetylcholine (Ach).(B) Ach is synthesized & released by small striatal neurons, upon which it has an Exitatory effect.(C) Dopamine (DA) is synthesized by the pigmented neurons of SNPc & it has Inhibitory effect on striatal neurons.(D) Dopamine is transported from SNPc to Corpus striatum via Nigrostriatal or Dopminergic tract.(E) There is functional equilibrium exists in the striatum between Ach & Dopamine in the normal physiological condition. PATHOPHYSIOLOGY IN PD
(F) In PD , there is a loss of pigmented neurons (neuromelanin) in SNPc. As a result , the DA cocentration in the corpus striatum is markedly decreased.(G) There is formation of Lewy Bodies in the remaining neurons.(H) LEWY BODIES are characteristic intracytoplasmic , eosinophilic inclusion bodies. These are circular in shape with the dens central “core” & clear peripheral “halo”.(I) There may also be a decrease in other Neurotransmitter like noradrenaline(NA), 5hydroxytryptamine(5HT),gamma –aminobutyric acid (GABA),Enkephalins & substance-P.
(J) Involvement of non nigrostriatal system :- Cell loss outside the Substantia Nigra involves the following major neuron groups :-(1) Midbrain– ventral tegmental area.(2) Pons– noradrenergic locus coeruleus.(3) Midbrain– serotonergic dorsal raphe nuclei.(4) Basal forebrain – cholinergic nucleus basalis of Meynert in substantia innominata.(5) Brainstem– peptidergic nuclei
(K) Alteration in noradrenergic & serotonergic system results in Depression in pt.(L) Neuronal loss in the nucleus basalis , locus coeruleus & ventral tegmental area causes Dementia.(M) Loss of somatostatin neurons in the cortex results in Alzheimer disease.
(1) IDIOPATHIC.(2) INFECTIONS :- encephalitis lethargica , AIDS, cryptococcal meningitis and Jacob-Creutzfeldt disease.(3) NEUROTOXINS :- 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine(MPTP)manganese carbonmonoxide, carbondisulphide, cyanide, methanol.(4) DRUGS TOXICITY :- (a) Neuroleptic drugs. (b) Antidepressant drugs. (c) Antihypertensive drugs.(5) METABOLIC DISORDERS :- disturbed calcium metabolism result in calcification in BG. AETIOLOGY
(6) VASCULAR DISORDERS :- atherosclerosis , hypertension.(7) HEAD INJURY :- RTA , punch boxers syndrome.(8) MULTIPLE SYSTEM DEGENERATION :- $ Alzheimer disease $ Shy Drager syndrome $ Progressive supranuclear palsy. $ Wilsosn’s disease $ Amyotrophic lateral sclerosis. $ Olivopontocerebellar atrophy. $ Huntington’s disease $ Hallervorden – Spatz disease. $ Strionigral degeneration. $ Cortico-basalganglionic degeneration.
(A) The diagnosis of PD is based on the clinical symptoms & signs.(B) Blood & CSF examination and cerbral imagin such as CT Scan , MRI are non cotributory in making the diagnosis of PD.(C) Positron Emission Tomography (PET) using fluorodopa has been useful in detecting loss of dopa uptake in the striatum . It shows 60% reduction of fluorodopa uptake.(D) Single Photon Emission Computerised Tomography (SPECT).(E) DNA Analysis :- mitochondrial complex 1 activity is reduced, alterations in DNA, Monoamine oxidase-B (MAO-B) activity increased. DIAGNOSIS
(F) The diagnosis is usually made on the basis of history & clinical examination. Handwriting samples, speech analysis, interview questions that focus on developing symptomatology & physical examination are used in the preclinical stage to detect early manifestations of the disease.(G) The diagnosis of PD can be made if atleast two of the cardinal features are present.(H) EMG may done to find out the level of rigidity & also to know the increase in the reaction time & movement time.
(A) PD is a progressive disorder but its rate of progression is variable.(B) Before L-dopa therapy 28% of pt. became severely disabled or died with in 5 yrs of diagnosis , 61% with in 10 yrs & 83% with in 15 yrs.(C) Following L-dopa therapy only 9% became disabled or had died at 5 yrs , 21% at 10 yrs & 37.5% at 15 yrs.(D) Death may occur from aspiration pneumonia ,septicemia from UTI, decubitus ulcer or from secondary causes like vascukar disease or neoplasia. PROGNOSIS
PHARMACOLOGICAL TREATMENT(A) Anticholinergics – Trihexyphenidyl , Bentropine.(B) Dopamine replacement – Levedopa , Carbidopa , Sinemet , Sinemet CR.(C) Dopamine agonists – Pergolide , Bromocriptine .(D) Amantadine.(E) MAOI-B – Seligiline. TREATMENT