Download

1 / 31
310 likes | 321 Views
Learn about the definition, types, global prevalence, legal status, and social norms of FGM, its impact on physical and mental health, and why it persists.

E N D
Faith and Peaceful relations Forum 18th October 2017 Female Genital Mutilation (FGM) Professor Hazel Barrett Centre for Trust Peace and Social Relations, Coventry University. h.barrett@coventry.ac.uk
Definition FGM is defined by WHO as: ‘all procedures involving the partial or total removal of the female external genitalia or other injury to the female genital organs for non-medical reasons.’ (WHO, 2008,4)
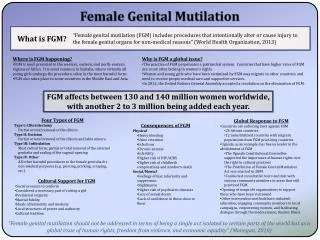
Female Genital Mutilation/Cutting Removal of clitoris and labia Scar tissue, cysts Damage to urethra, perineum, anal sphincter Fistula Inflexibility, tearing, inflammation on intercourse, difficulties in delivery Difficulty controlling urine Prolapse Post partum haemorrhage Greater susceptibility to infections Greater susceptibility to STI’s and HIV Painful sex Delivery problems Infertility Psychological problems, depression Foetal death Maternal mortality
FGM: global situation • FGM is a deep-rooted traditional practice that adversely affects the health and well-being of millions of girls and women. • Estimated that globally that 200mgirls and women have been subjected to FGM. • Practice is concentrated in 30 African, Middle Eastern and Asian countries. • Half of the women who have been subjected to FGM live in three countries: Indonesia, Egypt and Ethiopia • In 8 countries over 80% of women aged 15-49 have been subjected to FGM: Somalia, Guinea, Djibouti, Sierra Leone, Mali, Egypt, Sudan and Eritrea. • Each year 3m girls are at risk globally. (unicef, 2016)
Groupings of the 29 countries where FGM is concentrated, by FGM prevalence amongst girls and women aged 15-49. (adapted from Unicef, 2013, 27)
Percentage of girls who have undergone FGM/C, by type, as reported by their mother.(compiled from Unicef, 2013)
FGM is most commonly undertaken by traditional excisors although there is an increasing tendency for medicalisation. In Indonesia more than 50% of girls underwent FGM by a trained medical professional, it is higher in Egypt. • In majority of cases FGM is performed on girls before age 5, but can be at any time in a female’s life course. In Yemen 85% of girls were subjected to FGM within their first week of life. • Females can be re-infibulated throughout their lives, including after giving birth. Many women in Sudan and Somali have been subjected to FGM 5+ times. • In Nigeria female bodies are re-infibulated prior to burial.
FGM in the EU • EU Parliament believe FGM is a serious issue in Member States, such as the UK, which are home to significant numbers of migrants from high prevalence countries. In 2009 the EU Parliament estimated 0.5m women and girls in EU had been subjected to FGM. • A further 180,000 girls are at risk. • FGM is a criminal offence in most EU states. Many have extra-territoriality clauses.
FGM in the UK House of Commons Home Affairs Committee (July 2014): • Estimated that 170,000 women and girls are survivors of FGM in the UK • 65,000 girls aged 13 and under are at risk of FGM in the UK
FGM enhanced dataset in England FGM Types: Type 1 38% Type 2 31% Type 3 22% Type 4 9% Highest volume of cases: Somalia Eritrea Sudan Nigeria
UK Legal Situation concerning FGM In the UK FGM has been a criminal offence since 1985 (Female Circumcision Act). In 2003 legislation updated to address extraterritoriality(FGM Act). Serious Crime Act 2015 added a number extra additions, including anonymity for victims, parental responsibility, FGM POs and mandatory reporting.
Why is FGM practised? WHO FGM ‘Mental Map’ Source: WHO,1999, 7 • Continuation of FGM is motivated by a complex mix of interlinked sociocultural factors. • Beliefs associated with religion, hygiene and aesthetics and social acceptance combine to support decision-making in communities in favour of carrying out FGM.
Conceptual Model of Factors Promoting and Hindering FGM in Western CountriesSource: Berg et al, 2010
FGM is a Social Norm • FGM is a Social Norm • Individual’s actions are interdependent on the actions of others including family and wider community. ‘Even when parents recognise that FGM/C can cause serious harm, the practice persists because they fear moral judgements and social sanctions should they decide to break with society’s expectations. Parents often believe that continuing FGM/C is a lesser harm than dealing with these negative repercussions.’ (Unicef, 2010,3)
Findings suggest that there are at least 28 different terms used by the Somali and Sudanese communities to refer to the practice of FGM/C. These include: ‘Gudniin’ or ‘Gudnink’, ‘halal’, Heavy Sunna, Big Sunna, ‘Light Sunna’, ‘Small Sunna’, ‘Khatan’, ‘Pharoni’ and ‘Purification’. • Because of the ambiguous nature of the terminology used by communities, particularly the term ‘sunna’, makes it difficult to know what Type of FGM is being referred to. • The use of terminology is linked to the construction of identities in relation to ethnicity and belonging, with some individuals associating ‘FGM’ with the ‘West’. Terminology is also employed as a means to negotiate the complex powerrelations operating within the community. • Many of the British Somali participants associate FGM with Pharonic Circumcision (Type III). • A number of participants did not perceived ‘Sunna’ as ‘FGM’.
The terms which translate to ‘circumcision’ were the most frequently used. • Many of these terms, such as gudnin, kutari, khitan, and tahoor can be used to refer to both male and female circumcision. • This suggests that some communities equate female circumcision with male circumcision thus stressing the religious and hygiene aspects of the practice. • A Somali man living in the UK aged 18-23 explains: ‘Physical practice…for a woman…she’s …you know…cutting a bit of foreskin off her vagina…a little bit, not notnot a lot.’
The second most commonly used term was sunna, a word which translates as ‘blessings’ which has very strong religious links. • A Sudanese woman living in the UK aged 18-23 stated: ‘Sunna it’s the same thing as the man, like in Islam we do, we cut the begin things of the man, and the woman as well, just a tiny bit just to clean it that’s all, which is, it is something alright.’
Other terms, such as halaalayn and tahara stress the link between FGM and ‘purification’. • A UK Sudanese woman explains that she believes FGM is beneficial ‘for keeping women clean and eliminating bad smalls’.
The terms used for FGM Type III (infibulation) include pharanai tahoor and big sunna. • A Dutch Somali woman aged 60-65 described the practice: ‘In the pharonic one, the whole clitoral hood and both labias have been removed then they pour malmal (a traditional herb) and other flora in order to attach it together.’ • This type of FGM is clearly linked to societal expectations of female sexuality and is often justified on religious grounds. • It is interesting that this type of FGM was also referred to as the extreme, heavy or bad one and the old one, indicating that many members of these communities do not agree with the practice of infibulation (FGM Type III).
Sunna was viewed positively with women who have undergone sunna being regarded as ‘a good Muslim woman’. • As a Dutch Somali man aged 18-24 stated: ‘if she follows (has sunna) that it just shows that she’s more religious, she’s practising, she’s not fake……I see the one (that has sunna) as having a higher degree of faith to the one who doesn’t.’ • This last statement illustrates that the support for FGM is a matter of social convention which is reinforced by real or perceived community enforcement mechanisms.
Participants were aware of the negative impact of FGM on women’s physical, psychological and sexual wellbeing. • However, a number of participants suggested that ‘Sunna’ had very little negative impact. Indeed, a small number of participants suggested that FGM had health benefits, such as reducing the risk of cancer • Medicalisation of certain forms of FGM led to the belief that it did not pose a significant risk to women’s health and wellbeing • Young Somali men and women in the Netherlands were more aware of the issue than the young Somali men and women in the UK. Many of the Dutch Somalis noted that knowledge of FGM is high amongst the general population in the Netherlands, with FGM being associated with the Somali community. • There is a lack of communication between family members, particularly between the generations and genders, regarding FGM.
Mixed findings relating to legislation reducing individuals’ decision to practice of FGM both within the Sudanese and Somali community • Many of the UK participants claim to be unaware of the extraterritoriality clause • Some of the young Somali women believed that individuals who are circumcised outside the UK should not be prosecuted. • Most of the UK Somalis and Sudanese people interviewed believed that the sentence of 14 years was too much. • A number of participants reported that FGM does go on in both the Sudanese and Somali communities and that many people are not deterred by the law. • Dutch participants held the belief that FGM is widely practiced in the UK, despite the law. • A small number of UK and Dutch participants reported that young girls are taken from Holland to the UK to have FGM performed.
The UK’s first Female Genital Mutilation (FGM) webapp* aimed at young people in the UK Want to know more about FGM? Want to know what others are saying about FGM? Then ask Petals: http://petals.coventry.ac.uk Scan the QR code to visit the website *with built in privacy features
Petalsfor professionals: an app aimed at professionals who have FGM safeguarding responsibilities in the UKpetals.coventry.ac.uk/professionals • Many professionals know little about FGM. • Many professionals do not know or understand their legal responsibilities regarding FGM • Many do not know where to get help and advice.
‘FGM is illegal. It is child abuse and a form of violence against women and girls and therefore should be treated as such.’ (Multi-agency statutory guidance on FGM, 2016, 27) What actions can you take to end this practice? .
References • Barrett, H.R., Brown, K., Beecham, D., Otoo-Oyortey, N., & Naleie, S., 2011, Pilot toolkit for replacing approaches to ending FGM in the EU: implementing behaviour change with practising communities. REPLACE. Coventry University, Coventry. • Barrett, H, Brown, K, Alhassan, Y & Beecham, D, 2015, The REPLACE Approach: supporting communities to end FGM in the EU. A Toolkit. Coventry University, Coventry. • Barrett, H, Brown, K, Alhassan, Y & Beecham, D, 2015, The REPLACE Approach: supporting communities to end FGM in the EU. Community Handbook. Coventry University, Coventr • Cook, R.J., Dickens, B.M. & Fathalla, M.F., 2002, Female Genital Cutting (Mutilation/Circumcision): ethical and legal dimensions. International journal of Gynaecology & Obstetrics, 79, 281-287. • Dorkenoo, E., Morison, L, Macfarlane, A, 2007, A statistical study to estimate the prevalence of FGM in England and Wales. FORWARD, London. • EndFGM, 2010, Ending Female Mutilation: a strategy for the European Union Institutions. EndFGM, Brussels. • Equality Now, 2012, Female Genital Mutilation: Report of a research methodology workshop on estimating prevalence of FGM in England and Wales. 22-13 March 2012. Equality Now, London. • European Parliament (EP), 2009, European Parliament Resolution on Combating FGM in the EU. 24th March 2009(2008/2071(INI)). EU Brussels. • Morison, L., Scherf, C., Ekpo, G., Paine, K., West, B., Coleman, R., & Walraven, G., 2001, The long-term reproductive health consequences of Female Genital Cutting in rural Gambia: a community-based survey. Tropical Medicine and International health, 6 (8), 643-653. • Okonofua, F, 2006, FGM and reproductive health in Africa. African Journal of Reproductive Health, 10 (2), 7-9.
Population Reference Bureau (PRB), 2010, Female Genital mutilation/Cutting: data and trends. Available from : http://www.prb.org/pdf10/fgm-wallchart2010.pdf [accessed 3.2.11] • Royal College of Midwives (RCM), 2013, Tackling FGM in the UK. Royal college of Midwives, London. • Shaaban, L.M. & Harbison, S., 2005, Reaching the tipping point against FGM. The Lancet, 366, 347-349. • Toubia, N F & Sharief, E H, 2003, FGM: have we made progress? International Journal of Gynaecology and Obstetrics, 82, 251-261. • Unicef, 2007, Coordinated strategy to abandon Female Genital Mutilation/Cutting in one generation. Unicef, New York. • Unicef, 2010, Prevalence among women 15-49 as of 1st October 2010: Unicef global databases based on data from MICS, DHS and other national surveys, 1997-2009. Unicef, New York. • Unicef, 2013, Female Genital Mutilation/Cutting: a statistical overview and exploration of the dynamics of change. Unicef, New York. • UNFPA, 2007, A holistic approach to the ababndonment of FGM/cutting. UNFPA, New York. • UNFPA-Unicef, 2012, Joint Programme on Female Genital Mutilation/Cutting: accelerating change. Annual Report 2012. UNFPA-Unicef, New York. • WHO, 1999, Female Genital Mutilation: Programmes to date. What works and what doesn’t. Department of Women’s Health, WHO, Geneva. • WHO, 2000, A Systematic Review of the Health Complications of FGM. Department of Women’s Health, Family and Community Health, WHO, Geneva. • WHO, 2006, FGM and obstetric outcome: WHO collaborative study in six African countries. The Lancet, 367, 1799-1800. • WHO, 2008, FGM WHO Fact Sheet 241. Available from: www.who.int/mediacentre/factsheets/fs241/en/print.html [accessed 12.9.11] • WHO, 2011, An update on WHO’s work on FGM: Progress Report. WHO, Geneva