Download
1 / 43
500 likes | 1.1k Views
Faculty of Allied Medical Sciences Clinical Immunology & Serology Practice (MLIS 201). Typhoid fever. Prof. Dr. Ezzat M Hassan Prof. of Immunology Med Res Inst, Alex Univ E-mail: elgreatlyem@hotmail.com. Teaching Objectives. To define Typhoid Fever

E N D
Faculty of Allied Medical Sciences Clinical Immunology & Serology Practice (MLIS 201)
Typhoid fever Prof. Dr. Ezzat M Hassan Prof. of Immunology Med Res Inst, Alex Univ E-mail: elgreatlyem@hotmail.com
Teaching Objectives • To define Typhoid Fever • To know the causes and symptoms of the disease • To understand how the bacteria cause the disease • To know different methods to diagnose Typhoid fever • To define Widal test and its components • To describe the procedure of tube Widal test • To know how to interpret the results • To describe the procedure of slide Widal test • To know the causes of false +ve and flase –ve results • To know the limitations of the test
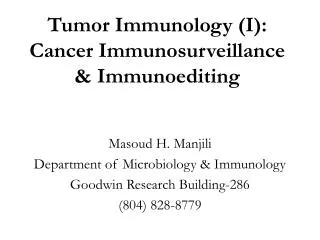
Countries endemic for typhoid (U.S. CDC 2006) Alex LaPointe, Wikimedia Commons
Definition • An infectious feverish disease caused by the bacterium Salmonella typhiand less commonly by Salmonella paratyphi. • The infection always comes from another human, either an ill person or a healthy carrier of the bacterium. • Persons with typhoid fever carry the bacteria in their bloodstream and intestinal tract • Transmitted through the ingestion of food or drink contaminated by the feces or urine of infected people • The bacterium can withstand both drying and refrigeration.
Causes 1. Caused by the bacterium Salmonella Typhi . 2.Ingestion of contaminated food or water. 3. Contact with an acute case of typhoid fever. 4. Contact with a chronic asymptomatic carrier.
Salmonella typhi • Rod shaped, flagellated, aerobic, Gram -ve bacilli. • Refrigeration and freezing could slow their growth. • Pasteurizing and food irradiationkill Salmonella for commercially-produced foodstuffs • Foods prepared in the home from raw eggs can spread salmonella if not properly cooked before consumption.
How does the bacteria cause disease ? Ingestion of contaminated food or water Salmonella typhi Carried by white blood cells into the liver, spleen, and bone marrow Multiply and reenter the bloodstream (Clinical illness) Bacteria invade the gallbladder, biliary system, and the lymphatic tissue of the bowel and multiply in high numbers Then pass into the intestinal tract (can be identified for diagnosis in cultures from the stool) Typhoid ulcers can cause perforation and hemorrhage
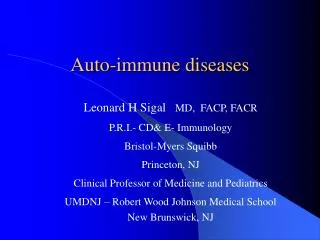
Symptoms • No symptoms - if only a mild exposure; some people become "carriers" of typhoid. • Poor appetite, Headaches and generalized pains, • Fever, Lethargy • Rose spots on chest wall • Diarrhea / constipation and abdominal pain • Chest congestion develops in many patients, • slow heartbeat. • Enlarged spleen and liver
Symptoms Rose spots Aches and pains High fever Diarrhea Chest congestion Typhoid Meningitis
Diagnosis Diagnosis of typhoid fever is made by • Clinical examination • Blood, bone marrow, or stool cultures for S. typhi • Serological Tests
Serodiagnosis of Typhoid : 1.Detection of Antibodies in serum: 1.Widal test (Tube or Slide), 2.Typhidot assay 3.Tubex system, 4. Dipstick assay. 2. Detection of Antigens in serum: 1. Tubex system 2. Countercurrent Immunoelectrophoresis (CIE). 3. Co-agglutination test. 4. ELISA 3. Detection of Antigens in urine: 1.Tubex system 2. CIE, 3. Latex agglutination 4. Co-agglutination
H( flagella ) antigens O (somatic) antigens Vi (Virulence) capsular polysaccharide antigens • Antigenic structure of Salmonella
O (somatic) antigens H (flagella) antigens • LPS in the cell wall; • Heat stable • Less immunogenic • Agglutination with antisera: • Fine, compact, granular chalky clumps • Present in flagella; • Heat labile; • Strongly immunogenic; Induce rapid & High Abtitres; • Agglutination with antisera: • Large, loose, cotton wool clumps
Vi (virulence) antigen • Capsular polysaccharide expressed on certain serotypes • Heat labile; • Poorly immunogenic, BUT antibodies are protective: • Detection of Vi antibody not helpful in diagnosis • Absence in a case of typhoid poor prognosis; • Persistence of Vi antibody : carrier state
WIDAL Test • Tube agglutination test. • Detects anti O and H antibodies in serum • Diagnosis of Typhoid and Paratyphoid cases • Carriers of typhoid bacilli possess antibody against the Vi antigen of S. typhi. (Vi tires seem to correlate better with the carrier state than do O or H titres). • For this reason, the use of Vi agglutination for detection of carriers was suggested . Dr.T.V.Rao MD
Widal test • Significance • I st week negative. • Titers raise in 2nd week • Raise of titers is diagnostic Dr.T.V.Rao MD
Materials • Antigens: • Suspension of S. typhi "O" antigen, O • Suspension of S. typhi "H" antigen; H • Suspension of S. paratyphi A "H" antigen, PA • Suspension of S. schottmuelleri "H" antigen, PB • Antibody: serum of suspected patient • Normal saline • Test tubes and pipettes
Saline 0.5 0. 5 0.5 0. 5 0. 5 0. 5 0. 5 1:10 Patient serum 0.5 0.5 0.5 0.5 0.5 0. 5 discard Serum dilution 1:20 1:40 1:80 1:160 1:320 1:640 - Bacteria suspension0. 5 0. 5 0. 5 0. 5 0. 5 0. 5 0. 5 PROCEDURE • Make the mark of tubes • Dilute patient’s serum 1:10 (0.1 ml serum + 0.9 ml saline). • Add reagents as the following: Reagent (ml)1 2 3 4 5 6 7 Final serum dil. 1:40 1:80 1:160 1:320 1:640 1:1280 -ve Bacteria suspension: O H PA PB Shake several times, put it in 370C water bath for 16-18 hours. Then let it stand at room temperature over night.
Observation: **Do not shake tubes before reading the results 1. Control tube (Tube No. 7): no agglutination (-) 2. Lowest titer tube: absolutely agglutination (++++) 3. Other tubes: ¾ agglutination(+++) ½ agglutination (++) ¼ agglutination (+) no agglutination (-) Interpretation: Agglutination titer: the highest dilution of serum which appears (++) bacteria agglutination.
H Agglutination how it appears after reactivity O Dreyer’s tube Conical bottom H agglutination Felix tube Round bottom O agglutination Compact granular agglutination Loose Cotton woolly clumps • Observed for agglutination: • H : Loose , cotton woolly clumps; • O : Compact Fine granular agglutination; • Supernatant should be clear;
How do you read Widal test results for typhoid fever? • The highest dilution of the patients serum in which agglutinations occurs is noted, ex. if the dilution is 1 in 160 then the titer is 160. • Agglutination in dilution up to <1:60 is seen in normal individuals . Agglutination in dilution 1:160 is suggestive of Salmonella infection. • Agglutination in dilution of >1:320 is confirmatory of Enteric fever .
Conclusion 1 2 3 4 5 6 7 O ++++ ++ ++ + - - - H ++++ +++ ++ ++ - - - PA ++ + - - - - - PB - - - - - - - 1:40 1:80 1:160 1:320 1:640 :1280 Negative control • N.B. • Single test not diagnostic (Except at high titers > 320). • Paired samples tests with rising titer is diagnostic • Diagnostic. • O > 1 : 80 • H > 1 :160 • H agglutinins appear first
Prozone phenomenon in Agglutination tests Prozone effect - Occasionally, it is observed that when the concentration of antibody is high (i.e. lower dilutions), there is no agglutination and then, as the sample is diluted, agglutination occurs. Lack of agglutination in the prozone is due to antibody excess resulting in very small complexes that do not clump to form visible agglutination
Limitation of Widal Test • The Widal test is time consuming and often times when diagnosis is reached it is too late to start an antibiotic regimen. • In spite of several limitation many Physicians depend on Widal Test Dr.T.V.Rao MD
Interpretation of Widal test • Test results need to be interpreted carefully in the light of : • Past history of enteric fever, • Typhoid vaccination, • general level of antibodies in the healthy populations in endemic areas of the world.
False Positive Reactions with WIDAL Test • patients who have had previous vaccination or infection with S typhi. • Cross-reaction with non – typhoidal Salmonella. • in association with some autoimmune diseases. • Infection with malaria
False Negative Reactions with WIDAL Test • Early treatment, • Relapses of typhoid fever. • Occasionally the infecting strains are poorly immunogenic.
Typical Serological Profile After Acute Infection Note that during Reinfections, IgM may be absent or present at a low level transiently
Slide Widal test: • Slide Widal test is more popular as it gives rapid results. Qualitative test: 1 drop of undiluted patient’s serum sample for the 2 antigens is placed on the circled card. 1 drop of each of 2 salmonella antigens are added separately rotated gently for 1 min. Appearance of agglutination gives qualitative results. (semiquantitative test is repeated with dilutions of serum)
Slide Widal test (Cont.): • Semi-quantitative test: 80µl, 40µl, 20µl, 10µl, 5µl, of patient’s serum each for 2 salmonella antigens are placed on the circled card. one drop of specific antigen is added to each series of serum. Agglutination of each of these is noted. Interpretation • 80µl corresponds to 1 in 20 dilution. • 40µl corresponds to 1 in 40 dilution. • 20µl corresponds to 1 in 80 dilution. • 10µl corresponds to 1 in 160 dilution. • 5µl corresponds to 1 in 320 dilution.
Prevention And Treatment
Prevention Two main typhoid fever prevention strategies: 1. Vaccination . 2. Avoid risky food and drinks
Medication Antibiotics • Antibiotics, such as ampicillin, chloramphenicol, fluoroquinolone trimethoprim-sulfamethoxazole, Amoxicillin and ciprofloxacin etc used to treat typhoid fever. • Prompt treatment of the disease with antibiotics reduces the case-fatality rate to approximately 1%.
Study Questions: • Write short note: Symptoms & Prevention of typhoid fever
Assigment • Write shortly on Widal test ميرنا ابراهيم – نادية محمد سعد – نيهال كمال – هايدى احمد – هدى عبد الله