Download
1 / 45
450 likes | 878 Views
ANEMIAS. Hemolysis. Hemolysis. Intravascular hemolysis. Rapid cell destruction Free Hb released in plasma Haptoglobin produced by liver Binds with free Hb and is degraded in liver Once Haptoglobins (Are reduced) are saturated, Free Hb is oxidised Methemoglobin + Albumin

E N D
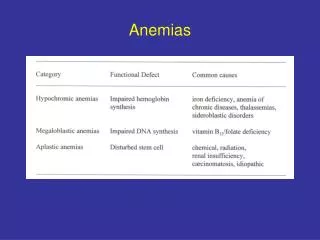
ANEMIAS Dr. Alka Stoelinga
Hemolysis Dr. Alka Stoelinga
Hemolysis Dr. Alka Stoelinga
Intravascular hemolysis • Rapid cell destruction • Free Hb released in plasma • Haptoglobin produced by liver • Binds with free Hb and is degraded in liver • Once Haptoglobins (Are reduced) are saturated, • Free Hb is oxidised • Methemoglobin + Albumin • Methemalbumin- degraded • Any Free Hb is bound to Haemopexin • If all of these mechanisms are saturated/ overloaded, Free Hb urine • When fulminant black urine (Falci. malaria) • In smaller amt Renal tubular cells absorb Hb, degrade it and store iron as hemosiderin • Subsequently tubular cells- sloughed- urine- hemosideriuria Dr. Alka Stoelinga
Extravascular hemolysis • Physiological Red cell destruction in RE cells in liver, spleen • Haptoglobulins are normal or slightly reduced Dr. Alka Stoelinga
Features of Hemolysis Blood film Spherocytosis No Spherocytosis Fragmentation • Hereditary • Enzymopathies DCT+ DCT- • Microangiopathic • Traumatic • Autoimmune hemolysis • Malaria • Clostridium • H. spherocytosis Dr. Alka Stoelinga
Congenital hemolysis • RBC membrane defects (hereditary spherocytosis/ Elliptocytosis) • G6PD deficiency • Hemoglobinopathies Dr. Alka Stoelinga
Red cell membrane defect • Defect in cytoskeleton • Usually due to quantitative or functional deficiency of one or more proteins in cytoskeleton • Cells loose their normal elasticity • Each time they pass through spleen, they lose membrane relative to their cell volume Raised MCHC Abnormal shape Reduced cell survival (EVH) Dr. Alka Stoelinga
Hereditary Spherocytosis • Autosomal dominant trait • 25% have no family history • Abnormalities in Beta spectrin and ankyrin Hemolytic crisis- when severity of hemolysis increases Megaloblastic crisis- follows folate deficiency Aplastic crisis- Parvovirus infection • Presents with severe anemia and low reticulocyte counts Dr. Alka Stoelinga
Investigations • Blood picture- presence of spherocytes • DCT –ve • Osmotic fragility test- Increased sensitivity to lysis in hypotonic saline solution Treatment • Folic acid prophylaxis 5mg once weekly • Blood transfusion after cross matching • Consider splenectomy • Growth retardation in children • Recurrent severe crisis • Death of a family member from the disease • Symptomatic cholecystitis Dr. Alka Stoelinga
G6PD deficiency • HMP shunt • NADPH – protects red cells against oxidative stress • G6PD deficiency Impairs production of NADPH • Affects male; females are carriers Clinical Features: • Acute drug induced hemolysis • Chronic compensated hemolysis • Infection or acute illnesses • Neonatal jaundice • Favism (Vicia fava/ broad beans) Dr. Alka Stoelinga
Investigations • Evidence of nonspherocytic intravascular hemolysis • Bite cells, blister cells, irregular small cells • Polychromasia reflecting reticulocytosis • If stained with methyl violet- denaturated Hb is visible as Heinz bodies within RBC cytoplasm • G6PD levels- low Treatment • Stop precipitating drugs • Acute transfusion support- life saver Dr. Alka Stoelinga
Autoimmune Hemolytic Anemia • Red cell autoantibodies RBC destruction • IgG/ M, rarely IgE or A CLASSIFICATION • Optimal temperature at which the antibody is active is used to classify AHA • 1. Warm antibodies • bind best at 37⁰C • Majority are IgG • React against Rh antigens • 80% of cases • 2. Cold antibodies • Bind best at 4⁰C but can bind upto 37⁰C • Majority are IgM and bind compliment • 20% of cases Dr. Alka Stoelinga
Warm autoimmune hemolysis • Middle aged females Causes • Idiopathic (50%) • Others Dr. Alka Stoelinga
Investigations • Hemolysis and spherocytes • DCT/ Antiglobulin test Treatment • Manage underlying condition • Stop offending drugs • Prednisolone 1mg/kg • Blood transfusion after cross matching • Splenectomy to be considered • Immunosuppressive therapy- Azathioprim/ Cyclophosphamide Dr. Alka Stoelinga
Cold Agglutinin disease • IgM binds red cells at 4⁰C and cause them to agglutinate • Low grade intravascular hemolysis- cold, painful, blue fingers, toes, ears, nose (acrocyanosis) • Blood film- red cell agglutination • MCV- raised • IgM Treatment • Keep extremities warm during winter • Steroids • Cross matching and blood transfusion Dr. Alka Stoelinga
The Direct Coombs test, is used to test for autoimmune hemolytic anemia. • In certain diseases or conditions an individual's blood may contain IgG antibodies that can specifically bind to antigens on the red blood cell (RBC) surface membrane, and their circulating red blood cells (RBCs) can become coated with IgG alloantibodies and/or IgG autoantibodies • Complement proteins may subsequently bind to the bound antibodies. • The direct Coombs test is used to detect these antibodies or complement proteins that are bound to the surface of red blood cells • Procedure: • A blood sample is taken and the RBCs are washed (removing the patient's own plasma) and then incubated with antihuman globulin (also known as "Coombs reagent"). If this produces agglutination of RBCs, the direct Coombs test is positive, a visual indication that antibodies (and/or complement proteins) are bound to the surface of red blood cells Dr. Alka Stoelinga
Hemoglobinopathies-Sickle cell anemia Dr. Alka Stoelinga
Hemoglobin • Hb has 4 globin chains • Each containing an iron containing porphyrin pigment called haem • Globin chains- 2α + 2non α chains • Hb A ααββ (90-97%) • HbF ααγγ (Fetus, 1%) • HbA2 ααδδ (2%) Dr. Alka Stoelinga
Abnormalities • Alteration in the amino acid structure of polypeptide chains of globin fraction of Hb • E.g.: Hb S • Amino acid sequence is normal but polypeptide chain production is impaired or absent • E.g. Thalassaemias Dr. Alka Stoelinga
Sickle cell anemia • Single glutamic acid Valine substitution at position 6 of beta globin polypeptide chain • Inherited as autosomal recessive trait • Homozygotes produce abnormal beta chains that make HbS/ SS • Results in clinical syndrome called Sickle cell disease • Heterozygotes produce a mixture of normal and abnormal beta chains that make HbA and HbS/ AS • Clinically asymptomatic sickle cell disease Dr. Alka Stoelinga
Pathogenesis • When Hb S is deoxygenated, molecules of Hb polymerize to form pseudocrystalline structures called Tactoids • These distort the RC membrane and produce characteristic sickle-shaped cells • Polymerization is reversible when reoxygenated • Permanent Distortion leads to Irreversibly Sickled red cells Dr. Alka Stoelinga
Note • Sickling is precipitated by: • Hypoxia • Acidosis • Dehydration • Infection • Irreversibly sickled cells have shortened survival • Plugs the vessels in microcirculation • This results in a no. of acute syndromes called crisis and chronic organ damage Dr. Alka Stoelinga
Clinical Features • Vaso Occlusive crisis (Most common) • Acute severe bony pain • Affects areas of active marrow • Hands and feet in children • Femora, humeri, ribs, pelvis and vertebrae in adults • Systemic response: • Tachycardia • Sweating • Fever Dr. Alka Stoelinga
Clinical Features • Sickle chest syndrome: • Follow vaso-occlusive crisis • Most common cause of death in Adult sickle cell disease • Bone marrow infarction leads to fat emboli to lungs • Ventilatory failure Dr. Alka Stoelinga
Clinical Features • Sequestration crisis • Thrombosis of venous outflow from organ • Loss of function • Acute pain • Spleen (Children) • Massive Splenomegaly severe anemia circulatory collapse death • Recurrent Sickling in spleen in children infarction • In adults No functional spleen • Capsular stretching Liver sequestration Severe pain Dr. Alka Stoelinga
Clinical Features • Aplastic crisis • Infection in adult sicklers with Parvovirus B19 • Results in severe but self limiting red cell aplasia • Very low Hb • Heart failure • Reticulocytes- “low” Dr. Alka Stoelinga
Investigations • Hb- low (6-8g/dl) • Blood film- sickled cells with target cells • Features of hyposplenism • Reticulocytosis • HbS (Na dithionite) • Hb electrophoresis • No Hb A • 2-20% Hb F • Predominance of Hb S Dr. Alka Stoelinga
Treatment • Prophylactic folic acid supplementation • Penicillin V • Pneumococcal, Haemophilus, hep B vaccination • Vaso-occlusive crisis • Aggressive rehydration • O2 • Analgesics • Antibiotics • Blood transfusion- full genotyped • Hydroxyurea Dr. Alka Stoelinga
Hemoglobinopathies-Thalassaemia Dr. Alka Stoelinga
Thalassaemias • Thalassaemia is an inherited impairment of hemoglobin production, in which there is partial or complete failure to synthesize a specific type of globin chain • In Thalassaemia the genetic defect, which could be either mutation or deletion, results in reduced rate of synthesis or no synthesis of one of the globin chains that make up hemoglobin. • This can cause the formation of abnormal hemoglobin molecules, thus causing anemia, the characteristic presenting symptom of the Thalassaemias. TYPES • α Thalassaemia • β Thalassaemia • Homozygous- Beta Thalassaemia major • β⁰- no β gene • β⁺- few β gene • Heterozygous- Beta Thalassaemia minor Dr. Alka Stoelinga
Pathophysiology • Normal hemoglobin is composed of two chains each of α and β globin. • Thalassemia patients produce a deficiency of either α or β globin, unlike sickle-cell disease which produces a specific mutant form of β globin. • The thalassemias are classified according to which chain of the hemoglobin molecule is affected. • In α thalassemias, production of the α globin chain is affected • In β thalassemia production of the β globin chain is affected. • β globin chains are encoded by a single gene on chromosome 11 • α globin chains are encoded by two closely linked genes on chromosome 16. • Thus in a normal person with two copies of each chromosome, there are two loci encoding the β chain, and four loci encoding the α chain. • Deletion of one of the α loci has a high prevalence in people of African or Asian descent, making them more likely to develop α thalassemias. • β thalassemias are common in Africans, but also in Greeks and Italians. Dr. Alka Stoelinga
α Thalassaemia • α thalassemias result in decreased alpha-globin production, therefore fewer alpha-globin chains are produced • Resulting in an excess of β chains in adults and excess γ chains in newborns. • The excess β chains form unstable tetramers (called Hemoglobin H or HbH of 4 beta chains) SUMMARY • Reduced or absent production of alpha chain • Chromosome 16 • 2 alpha gene loci • Hence, 4 alpha genes • If 1 is deleted- No clinical effect • If 2 are deleted- mild hypochromic anemia • If 3 are deleted- Hb H disease • If all 4 are deleted- Stillborn (Hydropfetalis) Dr. Alka Stoelinga
Complications Dr. Alka Stoelinga
β Thalassaemia • Mutations are characterized as (βo or β thalassemia major) if they prevent any formation of β chains (which is the most severe form of β thalassemia) • They are characterized as (β+ or β thalassemia intermedia) if they allow some β chain formation to occur. • In either case there is a relative excess of α chains, but these do not form tetramers: rather, they bind to the red blood cell membranes, producing membrane damage, and at high concentrations they form toxic aggregates SUMMARY • β Thalassaemia • Homozygous- Beta Thalassaemia major • Either unable to synthesize Hb A OR • Profound hypochromic anemia • β⁰- no β gene • β⁺- few β gene • Heterozygous- Beta Thalassaemia minor • Mild anemia • Little or no clinical disability Dr. Alka Stoelinga
Delta (δ) thalassemia • As well as alpha and beta chains being present in hemoglobin about 3% of adult hemoglobin is made of alpha and delta chains. • As with beta thalassemia, mutations can occur which affect the ability of this gene to produce delta chains. Dr. Alka Stoelinga
Functions of spleen Red pulp • Mechanical filtration of red blood cells • Reserve monocytes White pulp • Active immune response through humoral and cell-mediated pathways. Dr. Alka Stoelinga
Hematological malignancies Dr. Alka Stoelinga