Download
1 / 41
410 likes | 425 Views
This chapter provides an overview of tuberculosis (TB) with a focus on the anatomical alterations of the lungs and the clinical manifestations associated with TB. It also discusses the diagnosis of TB through various methods such as tuberculin skin testing, acid-fast stain and sputum culture, and polymerase chain reaction (PCR). The chapter also covers nontuberculosis mycobacteria (NTM) and their role in mycobacterial infections.

E N D
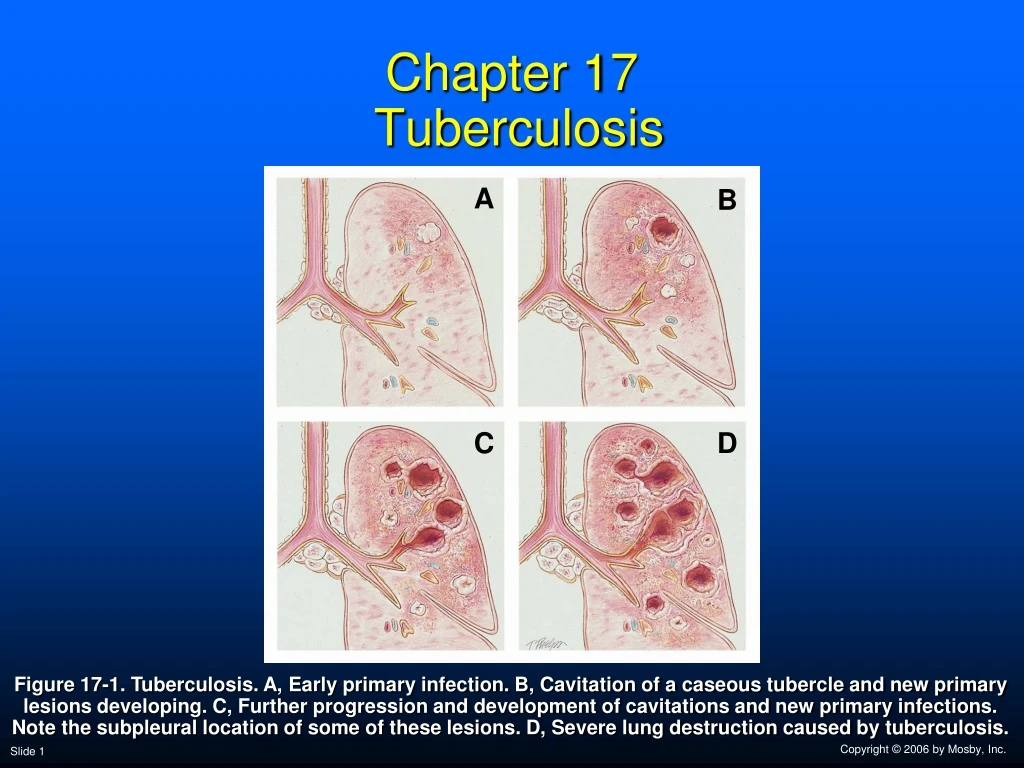
Chapter 17 Tuberculosis A B C D Figure 17-1. Tuberculosis. A, Early primary infection. B, Cavitation of a caseous tubercle and new primary lesions developing. C, Further progression and development of cavitations and new primary infections. Note the subpleural location of some of these lesions. D, Severe lung destruction caused by tuberculosis.
Anatomic Alterations of the Lungs (Three categories) • Primary tuberculosis • Primary infection stage • Postprimary tuberculosis • Secondary or reinfection TB • Disseminated tuberculosis • Extrapulmonary TB
Anatomic Alterations of the Lungs(Mainly Primary TB) • Alveolar consolidation • Alveolar-capillary destruction • Caseous tubercles or granulomas • Fibrosis and secondary calcification of the lung parenchyma • Distortion and dilation of the bronchi • Increased bronchial airway secretions
Etiology • In human, TB primarily caused by Mycobacterium tuberculosis • Others • Mycobacterium bovis • Mycobacterium ulcerans • Mycobacterium kansasii • Mycobacterium avium-intracellulare • Highly aerobic organisms
Diagnosis • Intradermal tuberculin skin testing • Mantoux test • Injection of purified protein derivative (PPD) • Wheal <5 mm: negative • Wheal 5 mm to 9 mm: considered suspicious • Wheal 10 mm or greater: positive
Diagnosis • Acid-fast stain and sputum culture • Ziehl-Neelsen stain • Reveals bright red acid-fast bacilli against a blue background • Fluorescent acid-fast stain • Reveals luminescent yellow-green bacilli against a dark brown background • A culture is necessary to differentiate M. tuberculosis form other acid-fast organisms • Results take as long as 6 to 8 weeks
Diagnosis • Identification of Mycobacterium species • Polymerase chain reaction (PCR) • Quick identification of organisms in expectorated or bronchoscopically obtained sputum • Deoxyribonucleic acid (DNA) probe
Nontuberculosis Mycobacteria • Mycobacterial infection caused by species other than M. tuberculosis are called nontuberculosis mycobacteria (NTM)—also called: • Mycobacteria other than tuberculosis (MOTT) • Atypical mycobacterial infection • Found in soil and water
Overview of the Cardiopulmonary Clinical Manifestations Associated with TUBERCULOSIS The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Alveolar Consolidation (see Figure 9-8), and Increased Alveolar-Capillary Membrane Thickness (see Figure 9-9)—the major anatomic alterations of the lungs associated with tuberculosis (see Figure 17-1).
Figure 9-9. Increased alveolar-capillary membrane thickness clinical scenario.
Clinical Data Obtained at the Patient’s Bedside Vital signs • Increased respiratory rate • Increased heart rate, cardiac output, blood pressure
Clinical Data Obtained at the Patient’s Bedside • Chest pain/decreased chest expansion • Cyanosis • Digital clubbing • Peripheral edema and distention • Distended neck veins • Pitting edema • Enlarged and tender liver
Digital Clubbing Figure 2-46. Digital clubbing.
DistendedNeck Veins Figure 2-48. Distended neck veins (arrows).
Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetes, ed 2,London, 1992, Mosby-Wolfe.
Clinical Data Obtained at the Patient’s Bedside • Cough, sputum production, and hemoptysis • Chest assessment findings • Increased tactile and vocal fremitus • Dull percussion note • Bronchial breath sounds • Crackles, rhonchi, and wheezing • Pleural friction rub • Whispered pectoriloquy
Figure 2-11. A short, dull, or flat percussion note is typically produced over areas of alveolar consolidation.
Figure 2-16. Auscultation of bronchial breath sounds over a consolidated lung unit.
Figure 2-19. Whispered voice sounds auscultated over a normal lungare usually faint and unintelligible.
Clinical Data Obtained from Laboratory Tests and Special Procedures
Pulmonary Function Study: Expiratory Maneuver Findings FVC FEVT FEF25%-75% FEF200-1200 N or N or N PEFRMVV FEF50% FEV1% N N or N N or
Pulmonary Function Study: Lung Volume and Capacity Findings VT RV FRC TLC N or VC IC ERV RV/TLC% N
Arterial Blood Gases Mild to Moderate Tuberculosis • Acute alveolar hyperventilation with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 60 PaO2 PaO2 or PaCO2 50 40 30 PaCO2 20 10 0 Figure 4-2. PaO2 and PaC02 trends during acute alveolar hyperventilation.
Arterial Blood Gases Extensive Tuberculosis with Pulmonary Fibrosis • Chronic ventilatory failure with hypoxemia pH PaCO2 HCO3- PaO2 Normal(Significantly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation Chronic Ventilatory Failure 100 Point at which disease becomes severe and patient begins to become fatigued 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 PaCO2 Pa02 or PaC02 60 50 40 30 PaO2 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute or chronic ventilatory failure.
Acute Ventilatory Changes on Chronic Ventilatory Failure • Acute alveolar hyperventilation on chronic ventilatory failure • Acute ventilatory failure on chronic ventilatory failure
Oxygenation Indices QS/QT DO2 VO2 C(a-v)O2 Normal Normal O2ER SvO2
Hemodynamic Indices (Severe Tuberculosis) CVP RAP PAPCWP Normal CO SV SVICI Normal Normal Normal Normal RVSWI LVSWI PVRSVR Normal Normal
Abnormal Laboratory Testsand Procedures • Positive tuberculosis skin test (PPD) • Positive acid-fast bacillus stain of sputumand sputum culture
Radiologic Findings Chest radiograph • Increased opacity • Ghon’s complex • Cavity formation • Pleural effusion • Calcification and fibrosis • Retraction of lung segments or lobe • Right ventricular enlargement
Figure 17-2. Cavitary reactivation TB showing a left upper lobe cavity and localized pleural thickening (arrows). (From Armstrong P et al: Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.)
General Management of Tuberculosis Pharmacologic agents • Consists of 2 to 4 drugs for 6 to 12 months • First-line agents (first 9 months) • Isoniazid (INH) and rifampin (Rifadin) • INH most effective • Often supplemented with: • Ethambutol • Streptomycin • Pyrazinamide
General Management of Tuberculosis • Respiratory care treatment protocols • Oxygen therapy protocol • Bronchopulmonary hygiene therapy protocol • Hyperinflation therapy protocol • Mechanical ventilation protocol
Review • The protective cell wall that surrounds and encases the TB bacilli is called -? • Tubercle or granuloma • What is primary TB? • Reaction following first exposure to pathogen • Inflammation leading to alveolar consolidation • Formation of tubercle • Fibrosis and calcification, development of bronchiectasis
What is postprimary TB? • Reactivation of TB after initial infection has been controlled • What is dissemminated TB? • Infection that spreads to sites outside the lung via pulmonary lymphatic system or bloodstream • The presence of numerous small tubercles scattered throughout the body is called - ? • Miliary tuberculosis
How long can TB bacillus remain suspended in the air after a sneeze or a cough? • Several hours • What is a Ghon’s complex? • Combination of tubercles and hilarlymphadenopathy seen on CXR • Typical ABG’s from a patient with extensive TB and fibrosis would be describe as - ? • Chronic Ventilatory failure and hypoxemia
What hemodynamic indices reflect right-side heart failure in a patient with advanced TB? • Increased CVP • Increased RAP • Increased mean PA • Increased PVR • Increased RVSWI • What respiratory care treatments/protocols are used for TB? • O2 Therapy • BHT • Hyperinflation Therapy
True or False • Pleural space complications such as empyema and pneumothorax are common in patients with tuberculosis. • True • A positive reaction to the tuberculin skin test confirms that a patient has active tuberculosis • False • Tuberculosis commonly develops in the apices of the lungs • True