Download
1 / 34
460 likes | 1.27k Views
OBSTETRIC INJURIES TO GENITAL TRACT & OBSTETRIC SHOCK. Dr Samar Sarsam. OBSTETRIC INJURIES TO GENITAL TRACT RUPTURE UTERUS IT IS A MOST SERIOUS CONDITION It usually occur during labor, rarely during preg. Incidence 0.3%. Causes: -During preg: Weak scar

E N D
OBSTETRIC INJURIES TO GENITAL TRACT & OBSTETRIC SHOCK Dr Samar Sarsam
OBSTETRIC INJURIES TO GENITAL TRACT • RUPTURE UTERUS • IT IS A MOST SERIOUS CONDITION • It usually occur during labor, rarely during preg. • Incidence 0.3%. • Causes: • -During preg: • Weak scar • Previous classical c/s. • Previous hysterotomy, metroplasty, myomectomy, perforation. • Direct trauma to abdomen. • Congenital abnormality of the uterus
During labor: • Obstructed labor. • Intra uterine manipulation. • Forcible dilatation of cx. • Injudicious use of oxytocin. • Previous weak scar. • Grand multiparous women • Pathology: • -complete rupture • -incomplete rupture. • Depending on whether the peritoneal coat is torn or not • In Britain a weak scar is the commonest cause of rupture uterus, if the uterus is over distended, scar imperfectly sutured, sepsis, the placenta implanted over the scar, when the latest incision is made through the previous scar. • c/s in the lower segment may stretch gradually attenuated avascular fibrosis causing relative intraperitonial bleeding when the scar give way
Symptoms and signs: • Rupture through scar during pregnancy, history of previous operation, scar on skin, thin abdominal wall, tender sulcus, may be silent rupture, or severe pain, shock. • Rupture during labor, dramatic symptoms, not always there is difficult labor. • Spontaneous rupture during obstructed labor, signs of obstruction, exhausted mother, tearing pain, shock, vaginal bleeding. • On examination: presenting part high, fetus extruded out of the uterus, contraction cease. • Rupture after intra uterine manipulation. • Extensive cervical laceration. • Rupture by oxytocic drugs, risk more in multip. • Direct injury to abdomen
Prognosis: • Mortality higher in cases of obstructed labor. • Fetal death is also more in cases of obstructed labor than in rupture in previous scar. • Treatment: • Recognize disproportion. • High risk cases deliver at hospital. • Upper segment scar deliver by c/s • Improve general condition, blood, I.V fluid, morphine, operation. • Repair or hysterectomy. + tubal ligation. • Antibiotics • Electrolyte balance.
LACERATION OF THE CERVIX • Caused by precipitated labor, forceps application, rapid delivery of the after coming head in breech presentation, previous scar in cx. From previous injury may tear. • Minor laceration is asymptomatic. • Deep laceration causes severe he during and after 3rd stage of labor. • Treatment: • Suturing under G.A using interrupted catgut or vicryl inserted through the whole thickness of its wall. • We need sponge forceps to complete our work.
LACERATION OF THE PERINIUM AND VAGINA • There are four degrees of this type of injury: • First degree: it involves only the skin • Second degree: it involves the perineal body up to the anal sphincter, but not involving it with a corresponding vaginal tear. • Third degree: secondary tear with partial or complete disruption of the anal sphincter. • Fourth degree: third degree tear with anal epithelium. • Extensive tear in the vagina may occur without tear in the perineum so inspection is important. • Treatment of first and second degree tears: • By repair of all lacerations to prevent ay infection. • If not sutured the possibility of uterovaginal prolapse is increased. • Start suturing from apex of the vaginal tear using continuous or interrupted suture using catgut or dexon using local anesthesia,G.A,epidural.
Third and fourth degree tears: • Experienced obstetric surgeon, theater, G.A, or epidural. • Early suturing with good results, if delayed the operation is difficult and incontinence is more also use catgut or dexon. • Anal mucosa is 1st repaired with the knot inside the bowel lumen. • Anal sphincter with interrupted suture, the rest as in 2nd degree tear repair. • After care – daily wash with soap and water, dried, may need a catheter. • If bowel motion is –ve by the fourth day, use glycerin suppositories not oral liquid paraffin. • If infection occurs we remove the stitches, drain, antibiotics, bathing until granulation tissue occur then 2ndry suture.
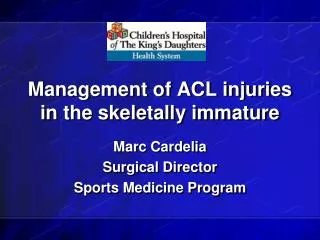
A first-degree laceration involves the fourchet, the perineal skin, and the vaginal mucous membrane. A second-degree laceration also includes the muscles of the perineal body. The rectal sphincter remains intact.
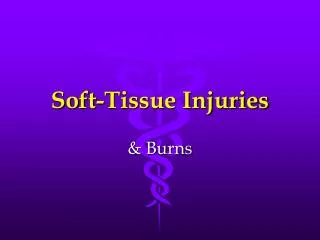
Layered primary closure of a fourth-degree obstetric laceration
VULVAL AND PARAVAGINAL HAEMATOMA • Divided into two types: • Supralevator hematoma • Infralevator hematoma • Infralevator: includes vulva, perineum, paravaginal, ischiorectal fossa. • Supralevator hematoma: it spread upwards and outwards beneath the broad ligament or partly downwards to bulge into the wall of the upper vagina and can track backwards into the retroperitoneal space. • Incidence: greater than 4 cm in diameter it occurs in 1/1000 deliveries. • Injury occurs with episiotomy. • In 20% of cases occur with intact perineum, • Half of women with genital hematoma have spontaneous delivery.
Diagnosis: • Usually obvious. • May be missed until shock occurs. • Symptoms: • Depend on rate and size of hematoma • Management: • Resuscitation, surgical evacuation if hematoma is larger than 5 cm or if expanding. • If small and not expanding, observation, ice-packs, antibiotics, analgesia.
SUBPERITONEAL HEMATOMA • Broad ligament hematoma, less common than genital hematoma. • It occur in 1 in 20000 deliveries. • They follow spontaneous vaginal or c/s or forceps. • 50 % discovered immediately, the other half 24 hrs later • presentation abdominal pain and hge. • Management: • Conservative. • If unstable homodynamic state do surgical exploration may need hysterectomy
FISTULA • - Due to prolonged pressure of the presenting part in prolonged labor, • -Or direct injury during operation, forceps. • Prolonged pressure causes ischemia then necrosis of anterior vaginal wall and base of bladder causing vesicovaginal fistula. • The rectum may also be involved, rectovaginal fistula commonly caused by complete tear. • If it is due to pressure necrosis it appears after 8 days when the slough separate. • Examination, opening is found. • Small fistula may heal in the rectum by granulation tissue healing. • But for vesicovaginal fistula this is unlikely. • If direct fistula direct repair. • If pressure fistula repair 2-3 months later.
MATERNAL NERVE INJURY DURING LABOR • -Foot drop from paralysis of dorsiflexor muscles of the leg may follow delivery. • In few cases it is due to pressure on lateral popliteal nerve near the neck of the fibula by a leg support • -In the majority of cases different type of injury involving the 4th and 5th lumbar nerve roots. • -Sudden prolapse of the intervertebral disc during labor, or pressure on the -----lumbosacral cord by the presenting part near the pelvic brim. • The lesion is usually unilateral and it follows difficult labor. • -Sensory loss, it follows footdrop and rarely follows epidural anesthesia.
OBSTETRIC SHOCK • Shock is a physiologic state characterized by a significant, systemic reduction in tissue perfusion, thereby resulting in decreased tissue oxygen delivery. • Three broad mechanisms of shock are recognized: • Hypovolemic — fall in intravascular volume • Cardiogenic — fall in cardiac output • Distributive, most often due to sepsis — fall in systemic vascular resistance
Shock may progress through a series of stages if not successfully treated, culminating in end-organ damage, irreversible shock, and death. • Irreversible shock seems to be associated with pooling of blood in the capillaries and tissues, leading to a further impairment in tissue perfusion. • The ensuing elevation in the capillary hydraulic pressure favors the movement of fluid out of the vascular space into the interstitium toxic products released from injured tissues or from the local accumulation of neutrophils can damage the capillary wall.
COMMON FEATURES OF SHOCK • Hypotension — Hypotension (systolic BP <90 mmHg) occurs in most shock patients. • Cool, clammy skin — In many shock states, regulatory processes compensate for decreased effective tissue perfusion. Potent vasoconstrictive mechanisms redirect blood from the periphery to the vital organs, thus maintaining coronary, cerebral, and splanchnic perfusion but causing the classic cool, clammy skin of shock. • Oliguria — • Other signs of hypovolemia in patients with shock include tachycardia, orthostatic hypotension, poor skin turgor, absent axillary sweat, and dry mucous membranes.
Change in mental status — • Metabolic acidosis — Initially, shock patients may have a respiratory alkalosis. However, as shock progresses, a metabolic acidosis develops, reflecting decreased clearance of lactate by the liver, kidneys, and skeletal muscle. If shock progresses to produce circulatory failure and tissue hypoxia, lactate production is increased due to anaerobic metabolism and can worsen acidemia.
Obstetrical shock • It does not differ from surgical shock; it results from depression of many functions. • Inadequate perfusion, oxygen depletion, accumulation of metabolites. • Hypotension without significant external bleeding may develop in an obstetric patient.
Causes: • 1-Concealed hge: any bleeding as in episiotomy, vaginal hematoma, rupture uterus with out obvious external bleeding leads to obstetric shock. • 2-Uterine inversion:has been discussed • 3-Amniotic fluid embolism • 4-septic shock • Diagnosis: • History • Examination • Manual exploration • If no cause is found think of coagulopathy. • Management: • Resuscitation • Oxytocic drugs • Removal and treatment of the cause
Amniotic fluid embolism: • This condition occurs when amniotic fluid enters the maternal circulation. • It causes cardio respiratory compromise as well as coagulation defect which is often severe. • Incidence and etiology: • 1 in 30000 pregnancies. • Associated with rupture membranes • Rapid labor • Vaginal delivery and c/s • Mechanism: access of amniotic fluid at higher pressure than usual into the maternal circulation through a defect some where near the placental site.
It is unpredictable and catastrophic consequences: acute cardiopulmonary embarrassment, coagulation failure. • Symptoms: • -Sudden onset of severe chest discomfort. • -Difficult breathing • -Pallor • -Cyanosis • -Cardiovascular collapse • Signs: • -Venous congestion with raised JVP. • -Output failure with tachycardia, hypotension, and peripheral vasoconstriction. • -Hge, coagulation failure, petechial skin hge. • -Bleeding at puncture site, vaginal bleeding. • -Coagulopathic signs may be the presenting features with out other symptoms.
Investigations: • -no time for investigations • -30 % will die in the first hr. • -suspicion when cardio respiratory collapse during labor or soon after delivery. • -diagnosis only confirmed at postmortem , by finding pulmonary vasculature packed with amniotic debris and trophoblast or aspirating blood from the pulmonary artery and examine for trophoblastic tissue. • -coagulation profile requested • Differential diagnosis: • Thromboembolism.
Management: • -Artificial ventilation • -Cardio pulmonary resuscitation • -Circulatory support • -I.V dopamine, steroids may be useful • -Correct acidosis • -Treat coagulopathy • -If the patient survive taken to the intensive care, anticoagulant, antifibrinolytics. • -fetus is unlikely to survive. • -after stabilizing the maternal condition vaginal delivery is preferable. • Prognosis: • Maternal mortality 90% • Prevention by avoiding excessive uterine contraction with oxytocin
VENOUS THROMBOEMBOLISM • IT IS A LEADING CAUSE OF MATERNAL DEATH • It occurs in 0.3% of pregnancies. • SEPTIC SHOCK: • Septic shock refers to a constellation of infection-mediated clinical findings marked by impaired vascular integrity resulting in inadequate tissue oxygenation and circulatory failure. Cellular hypoxia, organ dysfunction, and death ensue if the course of this process is left unaltered . • sepsis remains an important cause of maternal mortality in obstetrics, along with thromboembolism, hemorrhage, and hypertension .
PREGNANCY AND SEPTIC SHOCK — Pregnancy is traditionally considered an immunocompromised state. • Incidence — The incidence of bacteremia is approximately 8 to 10 percent in obstetric patients with clinical evidence of local infection. These patients rarely progress to more significant complications, such as septic shock. • Etiology — • Post-cesarean delivery endometritis • Endometritis following vaginal delivery • Urinary tract infections • Septic abortion • Intra amniotic infection • Necrotizing fasciitis • Toxic shock syndrome
Predisposing factors: • include prolonged premature rupture of membranes, cerclage in the presence of ruptured membranes, retained products of conception, pregnancy with a retained intrauterine contraceptive device, and instrumentation of the genitourinary tract. • Microbiology — The principal etiologic agents of septic shock are endotoxin producing aerobic Gram-negative bacilli, Gram-positive bacteria and mixed or fungal infections. Anaerobic organisms (eg, Bacteroides species, Fusobacterium, Peptostreptococci, Clostridium) are usually involved in mixed infections. • Prolonged hospitalization and use of broad spectrum antibiotics increase the risk of infection with resistant gram negative organisms and Pseudomonas sp. Anaerobes are part of the normal genitourinary and gastrointestinal flora, but may become pathogens when the normal mechanisms limiting their growth are altered. Antibiotics, decreased local vascular supply, foreign body material, and tissue trauma all favor anaerobic infection .
CLINICAL MANIFESTATIONS — The severity of the clinical presentation of sepsis is determined by the vigor of the host inflammatory response, rather than the virulence of the inciting infection • Early symptoms — Initial symptoms of sepsis may include malaise, nausea, vomiting, and, occasionally, profuse diarrhea. Bacteremia is typically manifested by shaking chills, a sudden rise in temperature, tachycardia, and warm extremities. Reductions in cerebral blood flow may cause abrupt alterations in mental status. Tachypnea or dyspnea result from a direct effect of endotoxin on the respiratory center and may immediately precede the clinical development of acute respiratory distress syndrome (ARDS). • Early in the course of shock blood pressure may actually be normal due to peripheral vasoconstriction; perfusion is disproportionately diverted from the renal and splanchnic circulations to maintain central blood pressure. The diagnosis of septic shock is often overlooked before hypotension occurs, although the woman may appear critically ill.
Late symptoms — Cold extremities, oliguria, and peripheral cyanosis are late manifestations in untreated and poorly responding cases. Myocardial depression becomes a prominent feature of prolonged septic shock, with marked reductions in cardiac output and systemic vascular resistance. Overt evidence of prolonged cellular hypoxia and dysfunction include profound metabolic acidosis, electrolyte imbalances, and disseminated intravascular coagulation (DIC). If these symptoms are left unabated, rapid progression to irreversible shock is the rule.
DIAGNOSIS — A careful physical examination and selected imaging studies are important in excluding uncommon sources. • The microbiological evaluation should include specimens from blood (at least two sets of blood cultures), urine, sputum, wound (in post-operative patients), and endometrium. • Both ultrasound and computed tomography (CT) imaging are helpful in searching for an intra abdominal abscess, retained products of conception, microabscesses in the myometrium, and septic pelvic vein thrombophlebitis. • Laboratory findings — • The white blood cell count may be depressed at first; however, a marked leukocytosis usually becomes evident. • A transient increase in blood glucose concentration due to catecholamine release and tissue underutilization is replaced by hypoglycemia when a reduction in gluconeogenesis subsequently occurs from hepatic dysfunction. • decreased platelet count, decreased fibrinogen concentration, elevated fibrin split products, and an elevated thrombin time. • Initial arterial blood gases may show a transient respiratory alkalosis from tachypnea, but metabolic acidosis develops as the lactic acid concentration increases from tissue hypoxia.
Management: • In pregnant women, priorities should first be directed toward maternal well-being, in spite of potential deleterious effects on the fetus. Improvements in the maternal status should have positive effects on the fetal condition since fetal compromise primarily results from maternal cardiovascular decompensation. • Volume expansion — • Vasoactive drug therapy —Dopamine is commonly used. • Oxygenation — • Antimicrobial therapy — • Empiric therapy in the septic patient should cover a wide variety of both aerobic and anaerobic Gram-negative and Gram-positive bacteria. A common antibiotic regimen is ampicillin (2 grams Q 4 hours), gentamicin (1.5 mg/kg Q 8 hours for patients with normal renal function), and clindamycin (900 mg Q 8 hours) or metronidazole (15 mg/kg initially then 7.5 mg/kg Q 6 to 8 hours). • Surgery —
COMPLICATIONS — Acute respiratory distress syndrome occurs as part of septic shock. • PROGNOSIS — Septic shock is a morbid event with high lethality