Download
1 / 18
220 likes | 473 Views
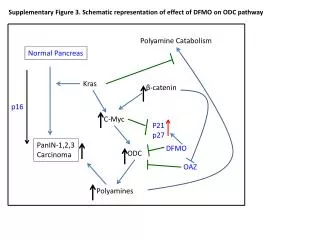
Mutation Screening of KRAS in FFPE samples using Pyrosequencing. Phil Chambers CR-UK Genome Variation Laboratory Service St. James’s University Hospital Leeds. Codon 12. Data from the Cancer Genome Project COSMIC database. Number of samples with mutations. Codon 13. Codon 61.

E N D
Mutation Screening of KRAS in FFPE samples using Pyrosequencing Phil Chambers CR-UK Genome Variation Laboratory Service St. James’s University Hospital Leeds
Codon 12 Data from the Cancer Genome Project COSMIC database Number of samples with mutations Codon 13 Codon 61 KRAS codon number KRAS • KRAS has 6 exons • Exon 1 is non-coding. Exons 2, 3, and 4 are invariant coding exons • Exon 5 undergoes alternative splicing • Mutation hotspots at codons 12 and 13 (exon 2) and 61 (exon 3)
KRAS • GTPase which plays a vital role in cell signalling • KRAS mutations play a role in many human cancers: • 15-30% lung adenocarcinomas • 20-50% colorectal carcinomas • Activating mutations cause KRAS to accumulate in the active, GTP-bound state
KRAS and monoclonal antibody therapy for colorectal cancer • More than 300,000 new patients are diagnosed with colorectal cancer (CRC) in the USA and European Union each year • Response rates, progression-free survival rates and overall survival have improved significantly in the last decade • Mainly as a result of: • New combinations of standard chemotherapy • New agents targeted at molecular events-small molecule inhibitors and monoclonal antibodies • Therapies directed towards epidermal growth factor receptor (EGFR) are of particular interest
KRAS and monoclonal antibody therapy for colorectal cancer • Chimeric immunoglobulin cetuximab: • Binds to EGFR and blocks ligand-induced phosphorylation • Is active in metastatic CRC expressing EGFR detected by IHC • Only 8-23% of patients achieved an objective response • Cancer Research 2006: v66, p3992-3995: • Presence of a KRAS mutation was significantly associated with the absence of response to cetuximab (0% of responders vs. 68.4% of non-responders; P = 0.0003) • Overall survival of patients without a KRAS mutation was significantly higher (median16.3 vs. 6.9 months; P = 0.016) • KRAS mutations are a predictor of resistance to cetuximab therapy and are associated with a worse prognosis
The EGFR signalling network Arteaga, C. L. Oncologist 2002;7(Suppl 4):31-39
What is Pyrosequencing? • Sequencing-by-synthesis technology suitable for analysing short-to-medium stretches of DNA • Assays give real-time quantitative results • Flexible assay design • Assays are simple and robust with inbuilt controls • Does not use fluorescent labels or gels/polymers
PCR primer Pyrosequencing primer Region of interest PCR primer Pyrosequencing assays • Three primers required: • Regular PCR primer • PCR primer with a 5’ biotin label • Sequencing primer • Two types of assay: SNP genotyping and sequence analysis (SQA) • Assay design favours short amplicons
Pyrosequencing workflow PCR Immobilisation – 5 minutes Isolation of ssDNA – 1 minute Annealing of sequencing primer - 2 minutes Pyrosequencing analysis – 10-60 mins/96 samples
Light Time Pyrosequencing technology PPi ATP
Quantitative SNP analysis heterozygote • Very short amplicon, therefore excellent for FFPE samples • Following ssDNA preparation, assay completed in 10 minutes • Straightforward data analysis using proprietary software • Table of peak heights can be exported for manual analysis heterozygote wild-type Reference peaks Negativecontrols Quantitative determination of mutant allele
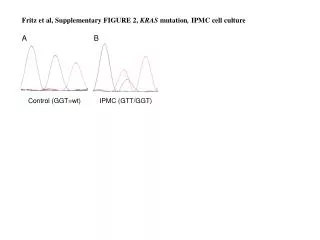
Quantitative sequence analysis c.35 G>A • KRAS codons 12 and 13 • Analysis of short - medium stretches of DNA • Assay design more challenging • Very short amplicon, therefore excellent for FFPE samples • Following ssDNA preparation, assay completed in 20 minutes • Table of peak heights exported for analysis in Excel WT Controls Reference peaks Quantitative determination of mutant allele
Spreadsheet-assisted analysis of sequence analysis data • Interpretation of sequence analysis data: • Done poorly by proprietary software, especially for diploid organisms • Inefficient and inaccurate when done by visual inspection • Low level variants are especially difficult to analyse • Assisted by calculation of peak height ratios and standard deviations peak heights >mean +1 standard deviation are also flagged if a variant is detected in this assay this peak height ratio will be <0.9, >1.1 spreadsheet-assisted analysis combined with visual inspection
Pyrosequencing summary • Flexible, simple assay design • Short amplicons • Straightforward data analysis • Quantitative • Rapid • Good quality control features • Self and mis-priming can be a problem • Accuracy of quantification calculations in homopolymer regions • Short read sequencing • Data interpretation in diploid organisms
Why is Pyrosequencing suitable for analysing KRAS in FFPE samples? • 90-95% of mutations occur in 2 hotspots • All mutations in each hotspot can be detected in one amplicon • Pyrosequencing favours short PCR amplicons • Problems caused by chemical modification of cytosine residues are not observed • Our data indicates the success of the technique
Mutation screening of KRAS in FFPE samples • KRAS mutation hotspots amplified in two amplicons: • codons 12 and 13: 80bp • codon 61: 86bp • Analysed using the Pyrosequencing SQA mode • 711 FFPE samples • DNA extracted using Proteinase K and phenol:chloroform • 43% (308/711) patients had a KRAS mutation • 0.7% (5/711) of samples failed analysis • 50 samples re-extracted with Qiagen DNA FFPE kit: • 1 failed analysis • no change in sensitivity and specificity of mutation detection • Similar data for other sample batches
Gene Collector Protocol overview(Fredriksson et al. NAR 2007, v35 p47) • Multiplex PCR (Pfu polymerase) • Blunt-ended products suitable for ligation by circularization • Collector probes guide circularization, closed circles formed by thermostable ligase • Enrichment of circular DNA by exonuclease treatment and rolling circle amplification
Acknowledgements • Cancer Research UK Genome Variation Laboratory Service Chris Booth Jo Lowery Helen Snowden Jo Morgan Graham Taylor • Leeds Institute of Molecular Medicine Susan Richman Sophie Grant Phil Quirke