Download
1 / 21
210 likes | 349 Views
Assessing and Monitoring of Nutrition as Therapy Done 8002. Shupikai Rinomhota Registered Nutritionist University of Leeds. Aim: To learn about assessment and monitoring of nutrition as therapy. Learning outcomes: At the end of the session, you should be able to:

E N D
Assessing and Monitoring of Nutrition as TherapyDone 8002 Shupikai Rinomhota Registered Nutritionist University of Leeds
Aim: To learn about assessment and monitoring of nutrition as therapy Learning outcomes: At the end of the session, you should be able to: • identify practitioners responsible for patients’ nutrition • assign responsibility for the assessment and monitoring of nutritional status • identify at risk patients • discuss the process of nutritional assessment • discuss monitoring and support of nutritional status
Who is at risk of malnutrition? 1 2 3 4 5 6 7 8 9
Factors that affect nutritional status Before hospitalisation (In the community)
Factors that affect nutritional status During hospitalisation: Patient factors:
Factors that affect nutritional status During hospitalisation: Institutional factors:
Factors that affect nutritional status Following discharge:
Assessment of nutritional status: There are several questions you have to answer: 1 What is nutritional assessment? 2 Who should do the assessment? 3 When should the nutritional assessment be done? 4 How should the nutritional assessment be done?
Actual Nutrient Intake The ability to eat is influenced by: a) Physical ability:- assistance/special cutlery b) Mouth:- dentition/ill fitting dentures c) GIT function:- diarrhoea, nausea, vomiting, constipation d) Emotional factors - loniliness/depression e) Pain:- uncontrolled pain affects appetite f) Food factors:- Unfamiliar meal patterns, palatability g) Physical environment:- hospital smells h) Social factors:- cultural/religious practices
Stages of Nutritional Screening (Reuben et al, 1995) Stage 1Stage 2Stage 3Stage 4 Nutritional Clinical requirements indices Risk factorsAnthropometricHealth measurementsoutcomes Dietary Intake Biochemical measurements
Nutritional Assessment - The Process A. Subjective Assessment i) Looking at the patient: What are you looking for? What does it tell you? • Under-weight---------- • Over weight------------ • Pallor-------------------- • Concave brittle nails-- • Sore tongue------------- • Cracked lips------------ • Bleeding gums--------- • Bruising easily---------
ii) Nutritional history It is important to take a nutritional history otherwise useful assessment data is lost: a) Have you intentionally lost weight recently? b) Have you been eating less than usual? c) What is your normal weight? d) How tall are you? Leonard-Jones et al (1995)
B Objective Assessment i) Anthropometric measurements: • weight (scales) • height • mid-arm circumference (tape) • triceps skinfold thickness (calipers) BMI (Quetelet Index) refers to Body mass Index BMI = Weight in kilograms (Height)2 in metres
ii) Biochemical measurements Prealbumin: Fe Status: Fe deficiency affects red cell indices producing reductions in MCV and MCH and Haemoglobin. Microcytic anaemia. B12 and folate status: Folate deficiency causes raised MCV and MCH. MCV = mean corpuscular volume MCH = mean corpuscular haemoglobin
Nutritional monitoring: Nurses: 1 Need to know how much food patients are eating. 2 Need to monitor weight changes in patients. 3 Need to recognize changes in clinical condition. Monitoring is an ongoing process.
Nutritional support Ethical considerations: Oral Feeding of patients: How can this be done with dignity and respect? Boosting calorific value: Olin et al (1994) enriched the lunches & dinners using ordinary food substances such as oil, cream, sour cream, butter, & milk. Desserts were enriched with cream or hydrolysed starch. What are your thoughts??
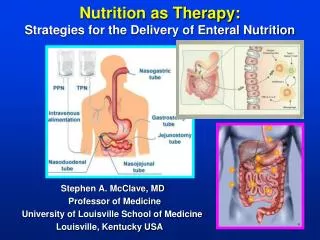
Nutrition as Therapy Methods available for nutritional support: 1 Normal foods Encourage patients to eat more Little and often 2 Enteral supplements: Small appetising snacks between meals Formulated liquid or semi-solid sip feeds 3 Enteral tube feeding: Directly into the stomach; PEG - percutaneous endoscopic gastrostomy (stroke) 4 Parenteral Nutrition:
Current NHS initiatives: 1 Benchmarking (2000) 2 NHS Better Hospital Food (2001)
Conclusions: 1. Nutrition plays a significant role in the health status of the patient. 2. There is increased demand on food components when people are ill. 3. Comprehensive nutritional assessment is desirable during admission. 4. Ongoing monitoring of actual food intake by patients is part of good practice. 5. Adequate nutrition is part of good therapy. Remember: “ If the GUT works, use it”
Useful References: Barnes KE (1990) An examination of nurses’ feelings about patients with specific feeding needs, J of Adv. Nursing, 15: 703-711 Bond S et al (1999) Eating Matters, Centre for Health Services Research, University of Newcastle upon Tyne Elmstahl S et al (1997) Malnutrition in geriatric patients: a neglected problem, J of Adv. Nursing, 26: 851-855 Holmes S (2000) Nutritional screening and older adults, Nursing Standard, September 27, Vol 15 (2): 42-44 Knaus WA, Draper EA et al (1985) APACHE II: a severity of disease classification, Critical Care Medicine, 13: 818-829 Norton B (1996) Nutritional assessment, Nursing Times, June 26, 92(26): 71-77
Useful References: Olin A O (1994) Energy-enriched hospital food to improve energy intake in elderly patients, Journal of Paremteral & Enteral Nutrition. 20(2): 93-97 Reilly H M et al (1995) Nutrirional screeining - Evaluation and implementation of a simple Nutrition Risk Score, Clinical Nutrition, 14: 269-273 Rinomhota S & Rollins H (2001) Energy balance, mood and behaviour (Part I), Nursing Times, 97(32):52-53 Rinomhota & Rollins (2001), Part II, NT, 97(44): 50-52 Romand J A & Suter P M (2000) Enteral nutrition: The right stuff at the right time in the right place, Critical care medicine, 28(7): 2671- Wood M & Creamer M (1996) Malnutrition in in Hospitals, Nursing Times, June 26, Vol. 92(26): 67-70