Download
1 / 1
10 likes | 118 Views
The Effect of Lecture and a Standardized Patient Encounter on Medical Student Rape Myth Acceptance and Attitudes Toward Screening Patients for a History of Sexual Assault Milone JM, Burg MA, Duerson MC, Hagen MG, Pauly RR. Introduction. Methods. Results. Discussion.

E N D
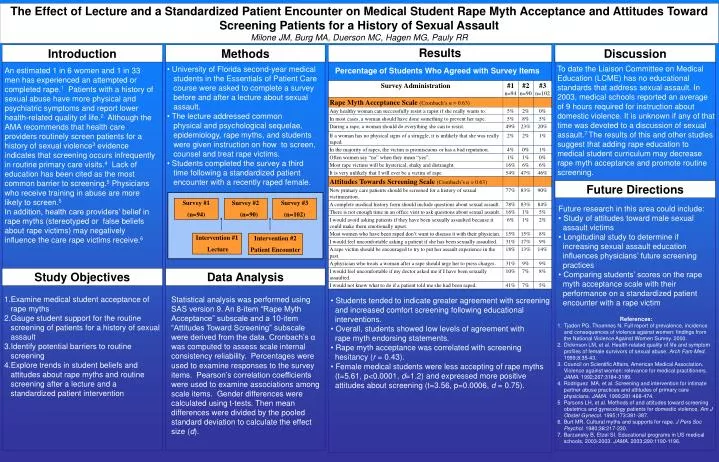
The Effect of Lecture and a Standardized Patient Encounter on Medical Student Rape Myth Acceptance and Attitudes Toward Screening Patients for a History of Sexual Assault Milone JM,Burg MA, Duerson MC, Hagen MG, Pauly RR Introduction Methods Results Discussion To date the Liaison Committee on Medical Education (LCME) has no educational standards that address sexual assault. In 2003, medical schools reported an average of 9 hours required for instruction about domestic violence. It is unknown if any of that time was devoted to a discussion of sexual assault.7 The results of this and other studies suggest that adding rape education to medical student curriculum may decrease rape myth acceptance and promote routine screening. • University of Florida second-year medical • students in the Essentials of Patient Care • course were asked to complete a survey • before and after a lecture about sexual • assault. • The lecture addressed common • physical and psychological sequelae, epidemiology, rape myths, and students were given instruction on how to screen, counsel and treat rape victims. • Students completed the survey a third • time following a standardized patient encounter with a recently raped female. An estimated 1 in 6 women and 1 in 33 men has experienced an attempted or completed rape.1 Patients with a history of sexual abuse have more physical and psychiatric symptoms and report lower health-related quality of life.2 Although the AMA recommends that health care providers routinely screen patients for a history of sexual violence3 evidence indicates that screening occurs infrequently in routine primary care visits.4 Lack of education has been cited as the most common barrier to screening.5 Physicians who receive training in abuse are more likely to screen.5 In addition, health care providers’ belief in rape myths (stereotyped or false beliefs about rape victims) may negatively influence the care rape victims receive.6 Percentage of Students Who Agreed with Survey Items Future Directions Survey #1 (n=94) • Survey #2 • (n=90) Survey #3 (n=102) • Future research in this area could include: • Study of attitudes toward male sexual • assault victims • Longitudinal study to determine if • increasing sexual assault education • influences physicians’ future screening • practices • Comparing students’ scores on the rape • myth acceptance scale with their • performance on a standardized patient • encounter with a rape victim Intervention #1 Lecture Intervention #2 Patient Encounter Study Objectives Data Analysis Statistical analysis was performed using SAS version 9. An 8-item “Rape Myth Acceptance” subscale and a 10-item “Attitudes Toward Screening” subscale were derived from the data. Cronbach’s α was computed to assess scale internal consistency reliability. Percentages were used to examine responses to the survey items. Pearson’s correlation coefficients were used to examine associations among scale items. Gender differences were calculated using t-tests. Then mean differences were divided by the pooled standard deviation to calculate the effect size (d). • Examine medical student acceptance of • rape myths • 2.Gauge student support for the routine screening of patients for a history of sexual assault • 3.Identify potential barriers to routine screening • 4.Explore trends in student beliefs and attitudes about rape myths and routine screening after a lecture and a standardized patient intervention • Students tended to indicate greater agreement with screening • and increased comfort screening following educational • interventions. • Overall, students showed low levels of agreement with • rape myth endorsing statements. • Rape myth acceptance was correlated with screening • hesitancy (r = 0.43). • Female medical students were less accepting of rape myths • (t=5.61, p<0.0001, d=1.2) and expressed more positive • attitudes about screening (t=3.56, p=0.0006, d = 0.75). • References: • Tjaden PG, Thoennes N. Full report of prevalence, incidence and consequences of violence against women: findings from the National Violence Against Women Survey. 2000. • Dickinson LM, et al. Health-related quality of life and symptom profiles of female survivors of sexual abuse. Arch Fam Med. 1999;8:35-43. • Council on Scientific Affairs, American Medical Association. Violence against women: relevance for medical practitioners. JAMA. 1992;267:3184-3189. • Rodriguez MA, et al. Screening and intervention for intimate partner abuse practices and attitudes of primary care physicians. JAMA. 1999;281:468-474. • Parsons LH, et al. Methods of and attitudes toward screening obstetrics and gynecology patients for domestic violence. Am J Obstet Gynecol. 1995;173:381-387. • Burt MR. Cultural myths and supports for rape. J Pers Soc Psychol. 1980;38:217-230. • Barzansky B, Etzel SI. Educational programs in US medical schools, 2003-2003. JAMA. 2003;290:1190-1196.