Download
1 / 145
1.48k likes | 1.91k Views
Learn about liver trauma, cancer, abscess, and bile metabolism. Discover surgical treatments, imaging methods, and postoperative care for liver and biliary diseases.

E N D
Disease of the Liver and Biliary Tract General Surgery Department dr Sigid Djuniawan, SpB
LIVER • HEPATIC TRAUMA • PENETRATING, BLUNT • Liver injury scale • Clinical : hypovolemic shock (hypotension, decreased urinary output, low cvp) • Imaging : Ct scan, FAST • Treatment : surgery • Complication : sepsis subhepatic (20%), hemobilia, stress ulcers Liver cancer • Hepatoma • Incidens : male= female, > 50 yo • Etiology : HVB chronic and HVC, aflatoxin, • Type : hepatoma, cholangiocarcinoma, hepatocholangioma (mixed) • Clinical : right upper quadran pain, reffered pain in shoulder, weight loss, jaundice (1/3 cases)
Clinical : hepatomegaly, arterial bruit, intermittent fever, ascites or gastriintestinal bleeding. • Laboratory : elevated bilirubin serum, increased alkaline fosfatase but serum bilirubin is normal (25%) • Imaging : CT scan, MRI, angiography • Liver biopsy (percutaneus core biopsy) • Tumor marker > 200 ng/ml • Treatment : partial hepatectomy, liver transplantation, ethanol injection, radiofrequency ablation. • HEPATIC ABCESS • Et : bacterial, parasitic, fungal • 90% right lobe= solitary, 10% left lobe = solitary • Cilinical : fever (high 40-41), jaundice unusual in solitary abcess, right upper quadrant pain and chills, malaise, fatique • Lab : leukocyte > 15.000, anemia, normal serum bilirubin • Imaging : atelectase in x rays, bof (air fluid level), usg and ct scan • Treatment : antibiotics Aminoglcosides, clindamycin, metronidazole, ampicillin), percutaneus catheter, lobectomy
METABOLISME BILIRUBIN HAEMOGLOBIN HAEM Bilirubin Non Conjugated globin Hepatocyte:Glucoronyl Transferase Bilirubin Conjugated HEPAR Ekskresi Empedu Urobilinogen Stercobilinogen
Biliary Tract • Biliary tract: Intra-hepatic bile duct Extra-hepatic bile duct Gallbladder Oddi sphincter From bile canaliculi to the ampulla of Vater
Intra-hepatic Bile Duct • Bile canaliculi • Segmental bile duct • Lobal bile duct • Hepatic part of left and right hepatic duct
Extra-hepatic Bile Duct • Left and right hepatic duct • The common hepatic duct Diameter :0.4-0.6 cm 2-4cm length • Common bile duct Diameter:0.6-0.8cm length:7-9cm • Gallbladder: the body,the fundus The neck • Cyst duct
Anatomy Calot triangle: • The triangle bounded by the common hepatic duct medially,the cystic duct inferiorly and the inferior surface of the liver superiorly is known as Calot triangle. • The fact that cystic artery ,right hepatic artery & para-right hepatic duct run within the triangle makes an important area of dissection during cholecytectomy.
Anatomy • The sphincter of Oddi: The proximal bile and pancreatic ducts and the common channel are surrounded by circular and longitudinal smooth muscle, this muscle complex is known as the sphincter of Oddi.
Special Investigation of the biliary Tract • Ultrasound: Non-invasive,painless, Easily performed First choice for biliary tract disease
Ultrasound • Bile duct stones: Stones in gallbladder: High echo which cast an acoustic shadow and which move with changes in posture
Ultrasound • Jaundice differential diagnosis: Dilatation of the ducts CBD: diameter > 1.0cm • Other disease: cholecytitis, tumor ect. • During surgery: to detect bile duct stones
Radiology • Plain abdominal radiograph: Radio-opaque gallstones Air in the biliary tree • Oral cholecystography: Biliary contrast medium A fatty meal
Radiology • Intravenous cholangiography • Percutaneous transhepatic cholangi-ography (PTC) show intra and extra hepatic biliary duct clearly complication: bile leakage cholangitis hemorrhage
Radiology • Endoscopic retrograde cholangio-pancreatography(ERCP) outline the biliary tree and pancreatic duct inspect the ampulla of Vater exam of the fluid of duodenum ,bile, pancreatic fluid.
Radiology • Endoscopic sphincterotomy(EST) • Endoscopic naso-biliary drainage (ENBD) • Computed tomography(CT) • Magnetic resonance cholangio-pancreatography (MRCP) • Cholangiopancreatography during & operation
Special Investigation of the Biliary Tract • Hepatobiliary nuclear imaging 99m-Tc-EHIDA • Choledochoscopy Operation Post opertion
Cholelithiasis • Including : gallstones biliary duct stones
Cholelithiasis In China: • before 1981 gallstones < biliary duct stones cholesterol stones < pigment stones • now gallstones > biliary duct stones cholesterol stones > pigment stones
Classification of stones • Cholesterol stones: hard,layed on cross-section • Pigment stones:crumble when squashed • Mixed stones: radio-opaque • Black stones
Formation of stones • Cholesterol stones: cholesterol insoluble in water and relative proportion of cholesterol,bile salts, and phospholipid in bile .
Formation of cholesterol stones • Increase of cholesterol and decrease of bile salts leads to supersaturation of bile with cholesterol ,which results in the formation of liquid crystalline phase of cholesterol
Formation of cholesterol stones • Nucleation:cholesterol will crystallize if there is a nidus on which the crystals can form. • Nucleating factors: mucus glycoprotiens from cyst wall and bilirubinate • Gallbladder function: the motility of the cyst wall
Formation of stones Pigment stones: • form of calcium bilirubinate • Bilirubin conjugated with glucuronide • β –glucuronidase produced by E. coli. can split the molecule • Unconjugated bilirubin precipitates as salt.
Gallstones (Cholecystolithiasis) Risk factor: • Women are three times more likely than men to develop stones • Obesity • Pregnancy • Dietary factors:high energy,low in fibre • Fasting
Risk factor of Gallstones • Biliary infection • Parasitic infestation • Diabetes mellitus • Gastric surgery • TPN • Cirrhosis of liver • Chronic haemolytic anaemia
Clinical feature of gallstones • 20-40% patient without symptom which is called asymptomatic gallstones • Chronic cholecystitis • Biliary colic • Acute cholecystitis
Symptoms • Gastrointestinal tract symptoms: upper abdominal discomfort, nausea, after meals, eap. fatty meals.
Symptoms Biliary colic: most commom symptom • A large or fatty meals and changing in position when sleeping can precipitate the pain • Due to impaction of stone in the neck of the gallbladder: the pressure increase. • Occurs in the mid or the upper-right portion of the upper abdomen. • Severe pain starts abruptly, continuous,with restlessness, vomitting,sweating. • Pain radiate to the right back and shoulder.
Symptoms Mirizzi syndrome: • Obstruction of the common hepatic duct by a stone impacted in the cystic duct or Hartmann’s pouch • Press on the bile duct or (more commonly ) ulcerate into the duct leads to cholecystocholedochal fistula
Mirizzi syndrome • Cholecystitis, cholangitis, and obstructive jaundice. • Cholangiography: narrow of the bile duct at the porta hepatis • Anatomy variation: cyst duct runs parallel to the hepatic duct
Symptoms Mucocele of the gallbladder: • A stone impacts in the cystic duct without bacterial infection • Bile is reabsorbed • The epithelium continues to secrete mucous,which is called “white bile”
Mucocele of the gallbladder • The gallbladder becomes distended • Easily palpable, maybe visible. • Infection does occur, an empyema may develop rapidly.
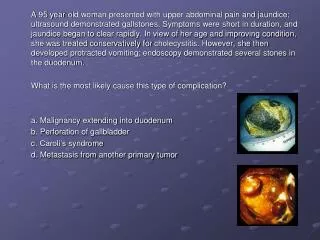
Symptoms Others: • Stones migrate through the cystic duct into the common bile duct: infection, jaundice. • Impaction of a small stone at the ampulla of Vater and occlusion of the pancreatic duct causes pancreatitis
Symptoms Others: • Cholecystoduodenal fistula intestinal obstruction • Gallbladder carcinoma
Sign • Right upper area of the abdomen tenderness, rigidity, rebound tendeness. • Gallbladder palpable • Murphy sign: inspiratory arrest during subcostal palpation • Jaundice:common bile duct stones or Mirizzi syndrome • Fever and chill with infection
Exam • Jaundice (choledocholithiasis): blood test of the liver function, elevation of the enzyme alkaline phosphate and bilirubin • WBC count is high • Ultrasoud: the main diagnosis exam. • Oral cholecytography.
Diagnosis • History • Physical exam • Ultrasoud exam: high echo with an acoustic shadow and moving with changes in posture (ductal dilatation), oral cholecystography (filling defect), BOF ( 10% radioopaque, pancreas calcification, porcelaine gall bladder) • Biliary tract : non ikteric : perioperatif cholangiography, ERCP) • Icteric : USG, ERCP, PTC)
Treatment • The first choice is operation: • symptomatic gallstones/ asymptomatic gallstones • acute/ chronic cholecystitis w or without gallstone • gallblader torsion • traumatic rupture • bilier peritonitis • carcinoma • retained stone Profilactic cholecystectomy : Stone > 2 cm Gallblader calcification
Treatment Asymptomatic gallstones: • oral cholecytography without showing of gallbladder • diameter of stones > 2.0-3.0 cm • diabetes mellitus • elder or cardiac and respiratory problems Need operation.
Treatment CBD exploration: Preoperation • CBD stones • Cholangitis and biliary colic repeatedly • Pancreatitis • Jaundice and bile duct dilatation
Treatment CBD exploration During operation • Cholangiography indicate CBD stone and bile duct dilatation • Palpable stones, ascarid, tumor • CBD diameter >1.0cm • Gallstone migrate into CBD • Pancreatitis • Draw out purulent or haematoid bile or bile with sandy stones