Download
1 / 34
350 likes | 657 Views
ASPIRIN ↓ Cox inhibition ↓ (PROSTACYCLIN) PGI 2 & TXA 2 (THROMBOXANE) LOW DOSE ASPIRIN. 1)PREVENT ARTERIAL THROMBOSIS IHD, STROKE 2) UNSTABLE ANGINA 3) RECENT MI 4) TIA 5) ARIFICIAL VALVES. 6) PTCA 7) PERIPHERAL ARTERIAL OCCLUSIVE DISEASE 8) CHRONIC LIMB ISCHEMIA. Aspirin ADR.

E N D
ASPIRIN↓ Cox inhibition↓ (PROSTACYCLIN) PGI 2 & TXA 2 (THROMBOXANE) LOW DOSE ASPIRIN
1)PREVENT ARTERIAL THROMBOSIS IHD, STROKE 2) UNSTABLE ANGINA 3) RECENT MI4) TIA 5) ARIFICIAL VALVES
6) PTCA 7) PERIPHERAL ARTERIAL OCCLUSIVE DISEASE8) CHRONIC LIMB ISCHEMIA
DIPYRIDAMOLE- VASODILATOR- THALLIUM IMAGING- INHIBIT PLATELET ADHESION TO VESSEL WALL↑ cAMP↓ PLATELET CALCIUM INHIBIT AGGREGATION + ASPIRIN – STROKE, TIA? SUPERIOR
CLOPIDOGREL & TICLOPIDINEINHIBIT ADP – INDUCED EXPRESSION OF PLATELET GP RECEPTORS↓DECREASE FIBRINOGEN BINDING↓DECREASE PLATELET AGGREGATION
CLOPIDOGREL → PRODRUG,TICLOPIDINE → NEUTROPENIA ↓ CBC – 2 WEEKS UPTO 3 MONTHS
THROMBOTIC STROKE SICKLE CELL ANEMIA ACS INTERMITTENT CLAUDICATIONPCI CHRONIC ARTERIAL OCCLUSION OPEN HEART SURGERY AV SHUNT
ABCIXIMAB • PCI + Aspirin & Heparin • in MI • Bleeding, thrombocytopenia, hypotension, Brady cardia
TIROFIBAN & EPTIFIBATIDE - Competitive, reversible inhibitors of fibrinogen binding to GPII b / III a - ACS – unstable angina, NSTEMI - Angioplasty & stenting - Bleeding
FIBRINOLYTICS: • Streptokinase Alteplase • Urokinase Reteplase • Anistreplase Tenecteplase
Streptokinase 1.5 million units over 60 minAlteplase 15mg bolus 0.75mg/1kg – 30 min0.5mg/kg- 60 min
Reteplase – 10mg bolus 10mg after 30minTenecteplase – IV bolus 0.5 mg /kg
HEMOSTATIC AGENTS:ε - Aminocaproic acid AprotininTOPICAL ABSORBABLE:Thrombin Microfibrillar collagen hemostat Absorbable gelatin Oxidized cellulose
THROMBOLYTIC THERAPYADV- Availability, rapid administration DISADV – Intracranial hemorrhage- Uncertainty of whether normal coronary flow has been restored- Reocclusion
Most effective within 12 hour (relative mortality decreased by 18%)- Little benefit beyond 12 hourNot for resolved chest pain, ST segment depression
Fibrin selective agents should be used with anticoagulants – UFH, LMWH, fondraparinux & bivalirudin Monitoring of thrombolytic therapy!
Persistent angina Persistent ischemic changes on ECG <50% Reduction in ST elevation 60-90 min after initiation of thrombolysis ---rescue PCI.
Routine coronary angiography & PCI within 24h of thrombolysis
Complications: Intracranial bleeding 0.7 – 0.9% Major bleeding requiring treatment 10% Venipuncture & arterial puncture.
Diagnosis of coagulation defects Prolonged APTT Defective Intrinsic Pathway No change in PT No change in APTT Defective Extrinsic Pathway Prolonged PT Prolonged APTT Defective in Common pathway Prolonged PT
Absolute C/I:1) H/o intracranial hemorrhagic / hemorrhagic stroke 2) Ischemic stroke within 3mo3) AVMs, aneurysms, tumor4) Closed head injury within 3 mo5) Aortic dissection6) severe uncontrolled HT – SBP > 180, DBP > 1107) Active bleeding / bleeding diathesis8) Acute pericarditis.
Intrinsic Pathway Extrinsic Pathway Tissue Injury Blood Vessel Injury Tissue Factor XIIa XII Thromboplastin XIa XI IXa IX VIIa VII Xa X X Prothrombin Thrombin Factors affected By Heparin Fribrin monomer Fibrinogen Fibrin polymer Vit. K dependent Factors Affected by Oral Anticoagulants XIII
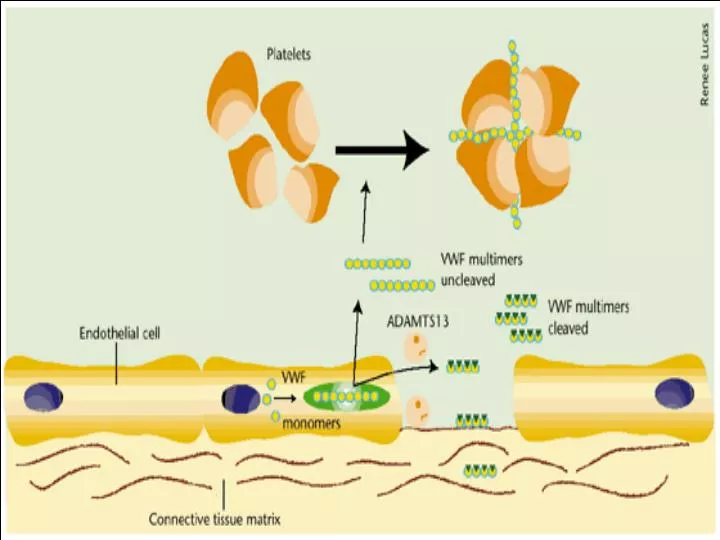
Thrombosis • Arterial Thrombosis : • Adherence of platelets to arterial walls - White in color - Often associated with MI, stroke and ischemia • Venous Thrombosis : • Develops in areas of stagnated blood flow (deep vein thrombosis), Red in color- Associated with Congestive Heart Failure, Cancer, Surgery.