Download
1 / 44
1.09k likes | 2.56k Views
DEHYDROEPIANDROSTERONE (DHEA). DR.T.RAMANIDEVI MD DGO FICS FICOG DIRECTOR, JANANI FERTILITY CENTRE RAMAKRISHNA NURSING HOME TRICHY. Introduction. 5-Dehydroepiandrosterone ( 5-DHEA ) 19-carbon endogenous natural steroid hormone

E N D
DEHYDROEPIANDROSTERONE (DHEA) DR.T.RAMANIDEVI MD DGO FICS FICOG DIRECTOR, JANANI FERTILITY CENTRE RAMAKRISHNA NURSING HOME TRICHY
Introduction 5-Dehydroepiandrosterone (5-DHEA) • 19-carbon endogenous natural steroid hormone • It is the major secretory steroidal product of the adrenal glands and is also produced by the gonads and the brain • DHEA converted to -50% of circulating testosterone in men -75% estrogen in women in perimenopausal age group - 100% in postmenopausal women
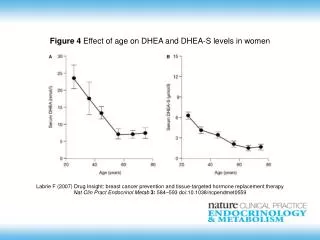
DEHYDRO EPIANDROSTERONE (DHEA) • Derived from cholesterol • Androgen precusor • Maximum concentration at 20’s • Decreases to 10-20 % by 80’s
DEHYDRO EPIANDROSTERONE (DHEA) CHOLESTEROL PREGNENOLONE DHEA DHEAS ANDROSTENEDIONE TESTOSTERONE OESTROGEN
DEHYDRO EPIANDROSTERONE (DHEA) • Supplements are made from substances called “Disogenin” • “Disogenin” is rich in soy and wild yams. • Only micronised forms of dhea are absorbed.
DEHYDRO EPIANDROSTERONE (DHEA) • Metabolised in liver • 50-70 % excreted by renal system • Half life : 7 - 38 min.
Mechanism of action Effect of Oral DHEA may be due to weak androgenic or estrogenic activity and to the fact that it is metabolized to androgens and estrogens NORMAL LEVEL OF DHEA – 80µg/dl to 320µg/dl
DEHYDRO EPIANDROSTERONE (DHEA) Low levels of DHEA is associated with • Ageing/ Alzhiemers • Obesity • Type II DM • Immune dysfunction • Autoimmune disease • Cancer
DEHYDRO EPIANDROSTERONE (DHEA) Low levels of DHEA is associated with • Depression • Loss of well being • CVS problems • Osteoporosis • Erectile dysfunction • Low libido • Infertility
1.DHEA TO IMPROVE OVARIAN FUNCTION Reprod Biomed Online. 2009 Oct;19(4):508-13.
2.Pre conditions the ovary for ovulation induction FERTILITY AND STERILITY SEP 2005
ACTION OF DHEAS PROHORMONE IMPROVES REDUCES OVARIAN APOPTOSIS RESERVE IMPROVES AUGMENTSOVARIAN IGF -1 ENVIRONMENT DHEA
Who require DHEA? • Women with • Physiological ovarian ageing ( all above age 40 ) • Premature ovarian ageing ( Below the age of 38)
DEHYDRO EPIANDROSTERONE (DHEA) Physiological Ovarian Ageing • All women above age of 40 with decreased fertility • Poor ovarian reserve due to age
DEHYDRO EPIANDROSTERONE (DHEA) Premature ovarian ageing • Function of the ovary is impaired • FSH level above 95 % tile • AMH below 95 %tile for her age
DEHYDRO EPIANDROSTERONE (DHEA) PREMATURE OVARIAN AGEINGTESTOSTERONE EVALUATED • UPPER 1/3 OF NORMAL • NO DHEA • LOW 2/3 OF NORMAL • DHEA GIVEN
3.ROLE IN POF/POI Increase in oocyte production after treatment with DHEA
DEHYDRO EPIANDROSTERONE (DHEA) • AMH – GOLD STANDARD ASSESSMENT OVARIAN RESERVE
DEHYDRO EPIANDROSTERONE (DHEA) • AMH increases in parallel with length of DHEA supplementation • This increase is more pronounced in younger POF than older DOR patients • Improvement in AMH levels predicts pregnancy success. Gleicher et al, rep.biomed online 2010.,
4.Reduces IVF cancellation rates • DHEA supplementation shows increase in IGF1 concentrations to potentiate gonadotrophin action in women with diminished ovarian reserves • Increase in average embryo scores per oocyte in IVF cycle outcomes and reduces IVF cancellation rates • DHEA supplementation facilitates gonadotrophins effect, it also reduces the dose of gonadotrophins in IVF cycles Hum Reprod. 2010 Oct;25(10):2496-500. Epub 2010 Aug 21. Hum Reprod. 2000 Oct;15(10):2129-32. Human reproductions sep 2006
Effect ofdehydroepiandrosterone on oocyte and embryo yields, embryo grade and cell number in IVF (Ref. 1 Human Reproduction 2006; 21: 2845-2849
5.Reduces miscarriage rates • DHEA supplementation has shown to have progestogenic effects in women with age related poor ovarian function to support conception and prevent miscarriages • DHEA augumentgonadotrophin secretionaugment HCG secretion to support corpus luteum for production of progesterone to support pregnancy • Overall reduces miscarriages and improve cumulative pregnancy outcome Fertility and sterility sep 2006
Miscarriage rates after dehydroepiandrosterone (DHEA) supplementation Ref. 1 Reproductive Biology and Endocrinology 2009, 7:108 )
Effect on pregnancy rate and speed of conception Control gp : 101 patients selected for IVF Study gp : 88 women with poor ovarian reserve evidenced by inadequately poor response to OI Conclusion : DHEA supplementation in women with diminished ovarian reserve, independent of age, leads to increased, and more rapid, conception rates DHEA 25mg TID for 3.7± 0.3 months Had IVF (microdose agonist/gn max 450-600IU 62 had IVF, 9 had atleast one prior OI, 17 missed Outcome –cumulative preg rate of 11 % IVF cancellation rate 26 % Miscarriages 44% Outcome – Cumulative preg rate of 27% IVF cancellation rate of 10% Miscarriages 24% Fertility and sterility vol 86,suppl 2, sep 2006
DEHYDRO EPIANDROSTERONE (DHEA) REPORTED REPRODUCTIVE BENEFITS • Improves egg/embryo numbers & quality • Spontaneous pregnancies • High IVF pregnancy rates • Shortens time to conceive • Cumulative pregnancy rates increases Barad et al,j Assist.rep. Genet 2007
DOSAGE FOR USE IN INFERTILITY • Administration of DHEA for 2 months 80µg/day increased the level of DHEA to 544+/- 55µg • Administration of DHEA ,four months prior to IVF cycles increases the response of the ovaries to gonadotrophin treatment and also improves the overall outcome Fertility and sterility sep 2005
DEHYDRO EPIANDROSTERONE (DHEA) Dosage - 25 mg three times a day - Stay with DHEA till pregnancy - Stop after pregnancy is confirmed
All patients with PCOS have increased senstivity to androgens upto 70% have elevated androgen levels and other 30% are in the high normal range • Hence initial conversion of DHEA to androgens does not favour its use • in treatment of PCOS Is there a role in PCOS ?
DEHYDRO EPIANDROSTERONE (DHEA) ROLE IN PCOs Poorly responding PCOS Where testosterone is decreased Better response with DHEA
OUTSIDE INFERTILITY • Used in HSDD (100mg twice daily for 6 weeks ) • Increases the bone mineral density in postmenopausal women • Improving symptoms of depression, schizophrenia and slowing the progress of Alzheimer’s diseases • Treating SLE- Increased E2 and reduced DHEAS levels in lupus patients may help induce cytokine abnormalities early in disease
CLINICAL APPLICATION DHEA
1.HOW IS IT USED ? 2.WHEN IT IS ORDERED ? • Concentrations of DHEAS are often measured, along with other hormones such as FSH, LH, prolactin, estrogen, and testosterone, to help diagnose polycystic ovarian syndrome (PCOS) and to help rule out other causes of infertility, amenorrhea, and hirsutism • It may be measured when a woman presents with signs and symptoms such as amenorrhea, infertility, and/or those related to virilization. These changes vary in severity and may include: • A deeper voice • Hirsutism • Male pattern baldness • Muscularity • Acne • Decreased breast size • DHEAS levels may be ordered, along with other hormones, to investigate and diagnose the cause of precocious puberty in young boys.
3.WHAT DOES THE TEST RESULT MEAN ? • Normal DHEA and Androgens – adrenal gland functioning is normal a. In PCOS, DHEA is elevated or normal (b’coz primary androgens are from ovaries ) b. Rarely it may be normal in adrenal tumors, when it is not secreting the hormone • Elevated level of DHEA – Adrenal tumors an increased level of DHEA is not diagnostic.it usually indictaes further testing to pinpoint the cause of hormonal imbalance • Low level of DHEA- adrenal dysfunction or hypopituitarism
What dose is used? • The following doses have been studied in scientific research: In postmenopausal women and in elderly men: Doses of 25-50 mg daily are commonly used • For treatment of schizophrenia: Increasing doses of DHEA of 25 mg OD for 2 weeks, 25 mg BD for 2 weeks, and 50 mg BD for 2 weeks • For replacement of hormones when the adrenal glands are not working well (androgen deficiency): 25-50 mg given daily as a single dose • For systemic lupus erythematosus(SLE): 200 mg per day along with conventional medical treatment, but doses up to 600 mg per day have been used • For improving bone mineral density in people with weak bones (osteoporosis): 50-100 mg per day • For erectile dysfunction: 50 mg per day
INTERACTIONS Anastrozole (Arimidex) Exemestane (Aromasin) Insulin Letrozole (Femara) Medications changed by the liver (Cytochrome P450 3A4 (CYP3A4) substrates) Some medications changed by the liver include lovastatin (Mevacor), ketoconazole (Nizoral), itraconazole (Sporanox), fexofenadine (Allegra), triazolam (Halcion), and many others. Tamoxifen (Nolvadex) Triazolam (Halcion) Medications for inflammation (Corticosteroids)- Decreases the effect of DHEA
SIDE EFFECTS • Acne • Hair loss • Stomach upset • High blood pressure. • Some women can have changes in menstrual cycle, facial hair growth, and a deeper voice after taking DHEADHEA is UNSAFE when used in larger amounts and long-term.
CONTRAINDICATIONS DHEA supplementation is contraindicated in those with breast, uterine, prostate and ovarian malignancy Liver diseases Pregnancy and breast-feedingHormone-sensitive conditions such as breast cancer, uterine cancer, ovarian cancer, endometriosis, or uterine fibroidsDiabetes Mood disorders Polycystic ovary syndrome (relative) Cholesterol problems
TAKE HOME MESSAGE • Improves ovarian function especially in poor responders • Prohormone – helps in preparation of ovaries before OI/ IVF • Increase the quality of oocytes and average embryo scores • Increases the oocyte production in POF/POI • Improves pregnancy outcome • Decreases the rate of miscarriages






![Kalis Keto [UPDATED 2019] - New Weight Loss Pills! Do They Work ...](https://cdn4.slideserve.com/8190726/kalis-keto-weight-loss-diet-reviews-price-where-dt.jpg)