Download
1 / 26
260 likes | 547 Views
Laparoscopic or “minimally invasive” surgery is a specialized technique for performing surgery. In the past, this technique was commonly used for gynecologic surgery and for gall bladder surgery. Over the last 10 years the use of this technique has expanded into intestinal surgery. In traditional “open” surgery the surgeon uses a single incision to enter into the abdomen.

E N D
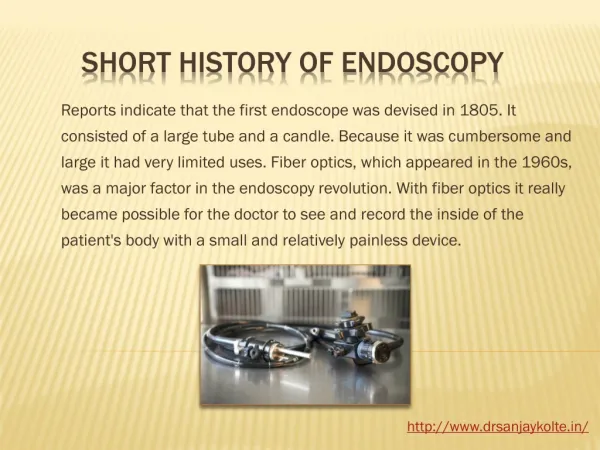
History 1902 - Georg Kelling, of Dresden, Saxony, performed the first laparoscopic procedure on dogs. 1910 - Hans Christian Jacobaeus of Sweden, reported the first laparoscopic operation on humans. 1980 - Patrick Steptoe from England, started to perform laparoscopic procedures in the operating room under sterile conditions. 1982 - The first solid state camera was introduced and this was the start of 'video-laparoscopy'. 1987 - PhillipeMouret performed the first video-laparoscopic cholecystectomy in Lyons, France. 1994 - A robotic arm was designed to hold the laparoscope camera and instruments. 1996 - The first ever live broadcast of laparoscopic surgery via the Internet was performed. http://www.drsanjaykolte.in/
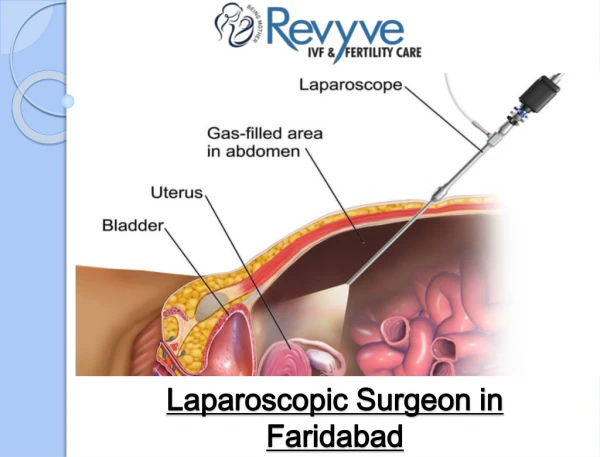
What is Laparoscopic Surgery? Laparoscopic surgery, also known as minimally invasive surgery (MIS) or ‘keyhole’ surgery is a modern surgical technique for carrying out operations in the abdomen through cannulae (also known as ports) which are channels into the body through small incisions. Using a video camera the surgeon is able to view the operative field without invasive surgery. The abdomen is usually insufflated with carbon dioxide gas. By inflating the abdomen, the abdominal wall is elevated above the internal organs to create a working and viewing space for the surgeons. http://www.drsanjaykolte.in/
Why Laparoscopy? There are a number of advantages to operating on the patient with laparoscopic surgery versus open surgery. Some of these are: Less post-operative scarring Reduced pain Shorter recovery time Less time spent in hospital to recover Reduced hemorrhaging Reduced risk of exposing internal organs to external contaminants Quicker return to normal activities Quicker return to work Reduced wound complications http://www.drsanjaykolte.in/
The Rise of Bariatric Surgery One of the most common types of laparoscopic surgery is bariatric (obesity). Over the last decade there have been more advancements in bariatric surgery than there had been in the previous 50 years, fuelled largely by the growing obesity epidemic which began in the 1970s. The epidemic created the need for effective treatment of severe obesity and its co morbidities leading to the development of procedures such as gastric banding, gastric bypass and duodenal switch over the past decade. More recently, the advent of minimally invasive surgery in the mid-1990s accounted for the second wave of advances. Before Laparoscopic Surgery Before laparoscopy was practiced, surgeons operated using open/invasive surgery. This means cutting skin and tissues so that the surgeon has direct access to structures and organs. This involves more direct access than in minimally invasive procedures as the openings are bigger so the internal organs are openly exposed. http://www.drsanjaykolte.in/
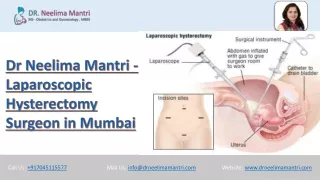
Laparoscopic Surgery Cholecystectomy, Appendectomy & Colectomy Vagotomy Hiatal, Inguinal & Diaphragmatic hernia repair Urological- Nephrectomy, Adrenelectomy & Prostatectomy. OBG-Tubal surgeries,cystectomies,hystrectomies & various ablations (endometriosis) Thoracoscopies Neurosurgeries Lumbar discectomies Diagnostic procedures http://www.drsanjaykolte.in/
Advantages and Disadvantages Advantages Minimal pain & illeus Improved cosmesis Shorter hospital stay , faster recovery & rapid return to work Non muscle splinting incision & less blood loss Post op respiratory muscle function returns to normal more quickly Wound complications i.e. infection & dehiscence are less Lap surgery can be done as day care surgery Disadvantages Longer duration of surgery Loss of 3D view, impaired touch sensation poor dexterity, fulcrum effect, risk of visceral / vsl. Injury (may go unrecognised) Long learning curve for surgeons http://www.drsanjaykolte.in/
Fig. Demonstarting surgical incision Sites in lap cholecystectomy http://www.drsanjaykolte.in/
INSUFFLATING GAS OF CHOICE FOR LAPROSCOPY Ideal insufflating gas of choice Colorless, non toxic, nonflammable, easily available, inexpensive, inert, readily soluble in blood and easily ventilated out of lungs Why CO2 is the gas of choice for laparoscopy? Nonflammable & does not support combustion Highly soluble in blood because of rapid buffering in blood so risk of embolisation is small Rapidly diffusible through membranes so easily removed by lungs CO2 levels in blood & expired air can be easily measured & its elimination is augmented by increasing ventilation CO2 is readily available & is inexpensive http://www.drsanjaykolte.in/
PROPERTIES OF OTHER GASES USED http://www.drsanjaykolte.in/
PHYSIOLOGICAL CHANGES Physiologic effects seen with CO2 insufflations are transient and derive from the body's reaction to increases in intra abdominal pressure and CO2 absorption as it tries to achieve a new state of homeostasis. People who are otherwise healthy will tolerate laparoscopy well, while individuals with underlying cardiopulmonary or renal diseases may not tolerate prolonged CO2 insufflations. Additionally, patient positioning, for example steep Trendelenburg in prostatectomy, can exacerbate cardiovascular alterations in laparoscopy. http://www.drsanjaykolte.in/
CARDIOVASCULAR RESPONSE Cardiovascular changes vary with intra abdominal pressure, with higher pressures associated with more significant changes than lower pressures. In any other case healthy patients undergoing laparoscopy, the threshold intra abdominal pressure that led to hemodynamic changes was 12 mm Hg. Those with underlying cardiac disease will likely have a lower intra abdominal pressure threshold. Heart rate may rise transiently in response to increases in SVR and arterial blood pressure level to maintain cardiac output, but most studies have reported no significant long-term changes in heartbeat with laparoscopy. In a tiny subset (0.5%) of otherwise healthy patients, however, bradycardia and asystole can occur during CO2 insufflation and pneumoperitoneum. http://www.drsanjaykolte.in/
RESPIRATORY RESPONSE CO2 may be the gas of choice for laparoscopic surgeries because it is noncombustible, extremely soluble, and readily eliminated with the lungs. Despite the proven effectiveness and protection of CO2 for insufflation in laparoscopy, the respiratory response to mechanical improves in intra abdominal pressure as well as hypercapnia from absorption should be considered. With CO2 insufflation and increases in intra abdominal pressure, the dintra abdominal pressurehragm is pushed cephalad into the thoracic cavity, constraining downward dintra abdominal pressurehragmatic excursion with respiration. All round functional respiratory capacity, vital capacity, and pulmonary compliance drop with boosts in intra abdominal pressure, and peak airway and plateau pressures can enhance up to 50% and 81%, respectively. http://www.drsanjaykolte.in/
RENAL RESPONSE Mechanistically, as intra abdominal pressure increases, its compressive effects on the renal vasculature, the renal parenchyma, and the IVC will reduce effective renal blood circulation (ERBF), cortical and medullaryperfusion, and renal venous outflow. The renal effects are mild to negligible once the intra abdominal pressure is under 10 mm Hg, but as intra abdominal pressure reaches and exceeds 15 mm Hg, there's a pressure-dependent decrease in the glomerular filtration rate (GFR), ERBF, creatinine clearance, sodium excretion, and urinary output. In a typical intra abdominal pressure of 15 mm Hg, urinary output decreases by as much as 63% to 64%, GFR by 21%, and ERBF by 26%. Despite this drop, however, there are no long-term renal squeal, even in patients with pre-existing renal disease, and pneumoperitoneum-induced renal failure does not occur. http://www.drsanjaykolte.in/
METABOLIC RESPONSE Metabolic acidosis from CO2 absorption is the primary derangement with laparoscopy. Systemic CO2 absorption and resultant metabolic consequences differ depending on the patient's underlying respiratory status since the lung eliminates absorbed CO2 buffered by the blood. In otherwise healthy patients, an increase in minute ventilation is enough, but for individuals with COPD, removal of CO2 is less capable, causing them to are afflicted by more major and extended derangements in acid-base balance. As stated earlier, desufflation might be necessary during a long laparoscopic procedure in patients with COPD or interstitial lung condition. http://www.drsanjaykolte.in/
Causes for Paco2 during Laparoscopy Absorption of carbon dioxide (CO2) from the peritoneal cavity VA/Q mismatch: Increased physiologic dead space Abdominal Distention Position of the patient (e.g., steep tilt) Controlled mechanical ventilation Reduced cardiac output These mechanisms are accentuated in sick patients Increased metabolism (e.g., insufficient plane of anesthesia) Depression of ventilation by anesthetics (e.g., spontaneous breathing) Accidental events CO2 emphysema (i.e., subcutaneous or body cavities) Capnothorax CO2 embolism (Selective bronchial intubation) http://www.drsanjaykolte.in/
ANAESTHESIA PAC Done in usual manner with special attention to cardiac & pulmonary system Investigations Complete hemogram RBS Na, K BUN, Creatinine Coagulation profile CXR, ECG BG, CM Special investigations ECHO PFT http://www.drsanjaykolte.in/
PREMEDICATION NPO Complete bowel preparation Antibiotics as per surgical team Awareness about post op shoulder tip pain Written informed consent for laparotomy Anxiolytics/antiemetics/H2 receptor antagonist/analgesic Antisialagogue(glyco-P) and vagolytic may be administered at induction of anaes. DVT prophylaxis (rTn, pelvic Sx, long duration, malignancy, obesity) Clonidine/ dexmetetomidine to decrease stress response http://www.drsanjaykolte.in/
MONITORING HR NIBP ContinousECG Pulse oximetry Capnography Temperature Airway pressure IAP If required, ABG, precordialdoppler,TEE may be instituted. http://www.drsanjaykolte.in/
CO2 s/c emphysema Cause accidental extraperitinsufflation (malpositionedverris needle) deliberate extraperit insufflations- retroperitsurg,TEPP,fundoplication, pelvic lymphadenectomy Diagnosis ETCO2 -cannot be corrected by adjusting ventilation even after plateau reached ABG, Palpation Treatment Stop CO2 insufflation, interrupt lap temporarily CMV continued till hypercapnia resolves Resume lap at low insufflation P thereafter http://www.drsanjaykolte.in/
Pneumothorax / pneumomediastinum Cause pleuroperitoneal communications (R>L) Diaph defects( aortic, esophageal, GE jnsurg) Rupture of preexisting bullae Perffalciform ligament Diagnosis – airway P, sudden ↓Sp O2 , sudden ↓/ ETco2, Abnormal motion of hemidiaph by laparoscopist PNEUMOTHORAX http://www.drsanjaykolte.in/
CO2 embolism (rare but potentially fatal) Risk factors hysteroscopies, previous abdsurg, needle/Trocar in vsl Consequences- GAS LOCK in vena cava ,RA → ↓ VR →© collapse - Ac RV HTN → opens foramen ovale → paradoxical gas embolism Diagnosis HR, ↓BP, CVP, hypoxia, cyanosis, ET CO2 biphasic change, Δa ETco2 ECG- Rt heart strain, TEE, pulm art. Aspiration of gas/ foamy bld from CVP line Treatment Release source (stop co2 + release pneumoperit) position – steep head low + durant position stop N2O + 100%O2 Hyperventilation CVP/PA catheter to aspirate CO2 Cardiac massage may break embolus- rapid absorption Hyperbaric o2 - cerebral embolism http://www.drsanjaykolte.in/
Endobronchial intubation Due to cephalad movement of diaph with head down tilt and IAP Diagnosis - Sp O2 ↓ airway P Treatment – Repositioning of ETT http://www.drsanjaykolte.in/
Aspiration Mendelson syndrome At IAP>20 mmHg Changes in LES due to IAP that maintain transsphincteric P gradient + head down position protect against entry of gastric content in airways http://www.drsanjaykolte.in/
Nerve injuries Prevented by avoid overextension of arms padding at P points http://www.drsanjaykolte.in/
Laparoscopy in children Physiological changes = adults Paco2 ETco2 increase but ETco2 overestimates Paco2 Co2 abs more rapid and intense due to larger peritoneal SA / body wt. More chances of trauma to liver during trocar insertion More chances of bradycardia , maintain IAP to as low as possible http://www.drsanjaykolte.in/
Laparoscopy in pregnancy Indications- appendicectomy cholecystectomy Risk – preterm labour, miscarriage, fetal acidosis Timing – II trimester (< 23 wk) Lap technique – HASSANS tech Special considerations prophylactic- antithrombolytic measures + tocolytics operating time to be minimised IAP as low as possible Continous fetal monitoring (TVS) Lead shield to protect foetus if intraopcholangiographyneeded http://www.drsanjaykolte.in/