Download

1 / 84
1.1k likes | 2.21k Views
Gram-negative Bacilli. Lectures 18-20. Gram-Negative Bacilli. The gram-negative bacilli are a highly diverse group of bacteria in many aspects Metabolism and growth Aeration requirements Substrates for metabolism and end products Virulence factors Large variance in enzymes and toxins

E N D
Gram-negative Bacilli Lectures 18-20
Gram-Negative Bacilli • The gram-negative bacilli are a highly diverse group of bacteria in many aspects • Metabolism and growth • Aeration requirements • Substrates for metabolism and end products • Virulence factors • Large variance in enzymes and toxins • They differ in the types of diseases they cause • They also differ in their pathogenicity • Primary pathogens • Opportunistic Pathogens
Gram-negative Bacilli • The gram-negative bacilli are diverse in the environmental niches they occupy • Some live in our intestines (enterics) • Some live in our respiratory tract • Some live in soil and water • Some are Zoonotic, meaning they cause diseases in animals that can be transmitted to us • All contain endotoxin • Important virulence factor • Causes all kinds of problems if too much in blood
Gram-negative Bacilli • Endotoxin role in disease • Stop cilia in respiratory tract • Initiate inflammation • Septic Endotoxin Shock • Kills 100,000 per year • Low blood pressure, lack of blood to organs • Multi-organ failure in severe • All due to inflammatory cytokine cascade • Protective usually, but overstimulation fatal • Anti-LPS and TNF drugs
The Gram-Negative Coccobacilli This group includes: Haemophilus influenzae Bordetella pertussis Francisella tularemia Brucella species Pasteurella multocida Similar in bacterial shape and Gram stain. However, they are very different with respect to: Diseases they cause and populations they infect Virulence Factors and Pathogenesis Their ability to infect animals as well as humans Invasive versus non-invasive pathogenesis
Haemophilus influenzae • Extracellular pathogen, does not invade into cells • Fastidious • This means it is difficult to grow • We must give it lots of growth factors • Haemophilus = blood loving • However, this organism can not grow on blood agar alone! • Requires X factor (hematin) • Requires V factors (NAD)
Haemophilus influenzae • Haemophilus influenzae strains can be divided into two groups based upon whether they produce a polysaccharide capsule • Encapsulated strains produce the capsule • Antibodies against the capsule show that there are 6 different serotypes (a-f) • Serotype B (Hib) causes 95% of invasive disease, meaning the bacteria enters the bloodstream • Almost all Hib cases are in young children • Unencapsulated strains don’t produce the capsule • They cause 90% of noninvasive respiratory tract infections • Especially when defenses are weak
Haemophilus influenzae • Virulence Factors • Haemophilus influenzae produce very limited known virulence factors • Fimbriae for attachment to respiratory tract cells • Capsule is produced to prevent phagocytosis • Endotoxin which is part of ALL Gram-negative cells • Helps respiratory tract colonization by blocking cilia clearance • Induces inflammation at site of infection • NO EXOTOXIN produced by H. influenzae • Causes disease by simply being in the environment and sparking inflammation through endotoxin
Haemophilus influenzae • Pathogenesis • Spread via respiratory droplets • Enters upper respiratory tract and throat and attaches to cells using fimbriae • Endotoxin stops respiratory tract cilia from beating and clearing the bacterial cells • Local spread (ears, sinuses, lungs) • Systemic spread (blood and brain) • Endotoxin and inflammation do the damage
Haemophilus influenzae • Systemic infections (meningitis) • Most prevalent in kids age 6 mos to 2 years • The key is protective antibody against capsule • Birth to 6 mos, maternal antibodies from mother protect children. However, after 6 months these maternal antibodies degrade • Can not make antibody to sugars 6 mos to 2 years so no protection from infection • 2 years on, make own antibody to sugars and start to make their own protection
Haemophilus influenzae • Systemic infections (meningitis) • Caused by encapsulated strains • Prior to the development of the new conjugate vaccines, 1 in 200 children got the disease • 65% of cases were in kids <1 year • 90% fatal untreated; 10% mortality treated • 33% long-term neurological defects possible even if properly treated
Haemophilus influenzae • Local Respiratory Tract Infections • Caused primarily by unencapsulated strains • A leading cause of infections in: • Ears, Sinuses, Lungs • Lung infections associated with weak defenses • Long-term smokers with COPD • Alcoholics have many defects in their lung defenses • Viral infections of lung (Influenza)
Haemophilus influenzae:Lab Diagnosis • Rapid diagnosis is critical in cases of meningitis • Every hour wasted is detrimental to the child • Conventional tests below can take 48 h to get answer • Gram-stain • Culture • Susceptibility • Rapid Identification methods were developed to get a quicker PRESUMPTIVE answer • These different test detect capsule antigen in spinal fluid • 15 minutes to 1 hour • Presumptive diagnosis only
Haemophilus influenzae • Treatment challenges • Up to the 1970s Ampicillin / Chloramphenicol were first-line drugs of choice, but then…... • Beta-lactamase (enzymes that inactivate ampicillin) in 35% of strains • Chloramphenicol resistance in up to 50% in some regions • Best drugs active against almost 100 percent of strains • Azithromycin (macrolide) • Fluoroquinolones • Newer Cephalosporin
Haemophilus influenzae • Prevention of meningitis • With antibiotic resistance increasing it is important to prevent infections before they start • 1980s capsule vaccine was not effective • Kids < 2 years old don’t make antibodies to sugars • Therefore, the most vulnerable went unprotected • 1990s scientist conjugated capsule sugar to a protein • Children under 2 can produce antibody to proteins • Also make antibody to the sugar attached to a protein • Started to vaccinate as young as 2 months old • Hib meningitis in children almost eradicated
Bordetella pertussis • Fastidious – hard to grow like H. influenzae • However, does not specifically require X and V • NOT INVASIVE, meaning never goes into the bloodstream. It does all its damage where it lands in the respiratory tract
Bordetella pertussis • Virulence Factors • Fimbriae for attachment like H. influenzae • Endotoxin role similar to H. influenzae • Big difference between the two is that Bordetella pertussis produces a bunch of different types of exotoxins • Pertussis toxin • Increases cAMP in lung cells • Increased cAMP = increased secretion • Excessive mucous and fluid build-up • Adenylate Cyclase Toxin • Also increases cAMP • Dermonecrotic Toxin • Tracheal cytotoxin
Bordetella pertussis • Pathogenesis • Respiratory droplet exposure • Enter respiratory tract • Attach to ciliated epithelial cells • Endotoxin inhibits cilia clearance • Replication on outside of respiratory cells • Cells eventually die and release toxin • This is an important point to understand when we talk about approaches to antibacterial therapy. The cells must die and release their toxins to cause the symptoms of the disease
Bordetella pertussis • Clinical Infection – Whooping cough • Epidemiology • Humans only reservoir • 60,000,000 cases annually world wide • 2000-6000 cases annually in US • Occur primarily in nonimmune children • Adults with waning immunity milder disease • Misdiagnosed as cold or flu
Bordetella pertussis • Three stages of Whooping Cough • Catarrhal stage • First stage as bacteria just start to die and release toxin • Mild cold symptoms, coughing, sneezing • Child is not that sick so parent thinks they have a common cold and don’t isolate from other children • This is the MOST contagious stage since many bacteria still alive in respiratory tract and all the coughing and sneezing spread live bacteria easily to other children
Bordetella pertussis • Paroxysmal stage • Maximum cell death and toxin release • Severe Cough • 40 – 50 cough spells/day • 20-30 coughs in a row with no chance to breath • Coughing causes stomach upset and vomiting • Mucous build-up in Lungs • Air blockage can in rare cases lead to death • Secondary pneumonia is biggest threat • Caused by other bacterial pathogens • H. influenzae, S. aureus, and S. pneumoniae
Bordetella pertussis • Convalescent stage • Coughing spells diminish slowly • decrease in number of spells and severity • Possible CNS complications in some children. The pathogenesis is not clear
Bordetella pertussis • Treatment • Self-limiting in majority of children • Supportive treatment • Antibiotics only speed up the process. • Erythromycin (Macrolides) • No effect on disease • Reduces number of live bacteria • Reduces the incidence of secondary pneumonia • Prophylaxis of contacts important
Bordetella pertussis • Vaccination (DPT – diphtheria, pertussis, tetanus) • Has own unique problems different from the H. influenzae • CNS toxicity was major stumbling block • Blamed on whole cell pertussis prep in the DPT vaccine • Many parents avoided vaccine and apathy led to wide spread outbreaks • New genetic engineered noncellular preparations have helped to alleviate fear in parents • However, only effective in 80-85% of children • Therefore, we still need to give antibiotics to contacts
Brucella species • Medically important species named for the livestock they commonly come from • Brucella abortus (cattle) • Brucella suis (pigs) • Brucella melitensis (goats) • General characteristics • Intracellular pathogen • Classic Zoonotic pathogen
Brucella species • Epidemiology • Worldwide prevalence • Causes serious problems in herds (abortions) • Routes of Transmission to humans are varied • Unpasteurized Milk (not a real problem in U.S.) • Slaughterhouse, veterinarians, livestock handler • Contact with infected tissue, blood, urine • Inhalation
Brucella species • Clinical syndrome (undulant fever) • Cyclic undulant fever that lasts for several weeks • Enlarged lymph nodes • Fatigue • Can be chronic long lasting • Diagnosis • Tough because clinical symptoms are so nonspecific • History of patient is most important • Where do they work • Where have the traveled (drank unpasteurized milk) • Difficult to culture (takes 6 weeks) • Looking for antibodies in serum also used to diagnose, but tricky
Brucella species • Treatment • Tetracycline is drug of choice • Bacteriostatic protein synthesis inhibitor • Good intracellular penetration • Relapses are still common though • Prevention • No vaccine for humans, some for animals • Kill infected animals and herds • 1000s in killed in Yellowstone National Park • Pasteurize milk and wear protective clothing
Francisella tularensis • General characteristics are very similar to Brucella species • Intracellular pathogen • Zoonotic
Franciscella tularensis • Epidemiology • Worldwide prevalence, widespread in U.S. • Found in >100 species of animals (RABBITS) • Insect vector important too, and is something we don’t see with Brucella • Routes of Transmission • Infected tissue (rabbit fever) • Inhalation • Ingestion • Insect bites
Franciscella tularensis • Clinical syndromes (depends on route of transmission) • Ulceroglandular • Most common form of disease (80% of cases) • Ulcer at site of inoculation • Commonly seen in hunters that kill rabbits and skin them • This would be the form seen from insect bite as well • Oculoglandular • Rub the eye and introduce bacteria into eye • Ulcers in conjuctiva of eye • Pneumonic • Highest mortality (10% if untreated) • Usually primary inhalation, secondary spread from other forms • Typhoidal • Ingested contaminated meat or water
Franciscella tularensis • Diagnosis • Clinical history of patient and symptoms • Did they hunt? Insect bite? Skin a rabbit? • Rarely cultured, hard to grow and dangerous to lab personnel • Treatment • Gentamicin (bactericidal)…..tetracycline alternative • Relapses common • Prevention • Protect against inoculation • Vaccination of lab personnel only
Pasteurella multocida • Similar general characteristics to Brucella and Francisella • Veterinary problem • Both domestic and wild animals • Respiratory/GI during stress (shipping fever) • Cholera in poultry • Hemorrhagic septicemia and pneumonia cattle • Human disease • Cellulitis from animal bites
Pasteurella multocida • Human disease • Cellulitis from animal bites • within 24 hours is key for differential diagnosis • Pneumonia from inhalation • Septicemia and death, this can occur in infants that are licked by infected dogs or cats in the face • Diagnosis and treatment • Patient history • Time of bite critical to differentiate from Gram positive pathogens that take longer to show symptoms • Penicillin very effective, rare for gram-negative bacteria
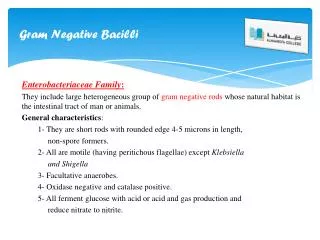
Enterics • We will now turn our attention to another diverse group of Gram-negative pathogens known as the Enterics • They are normally inhabitants of the gastrointestinal (GI) tract and some can actually be part of the normal flora • Some are members of the Enterobacteriaceae family • Escherichia coli • Salmonella species • Shigella species • Miscellaneous • Vibrio, Campylobacter, Helicobacter are other miscellaneous pathogens
Enterobacteriaceae • Morphology • Gram-negative rods, longer rods than the coccobacilli but still relatively short and fat • Growth Characteristics • Much easier to grow than the coccobacilli we talked about before • Habitat • Found most everywhere in nature (soil/water) • GI tract normal flora in humans • Upper respiratory tract (URT) in hospitalized which causes a lot of serious problems. Within a few days of going into the hospital the flora in the upper respiratory tract changes from streptococci and other gram-positives to gram-negative enterics that can cause serious infections and are usually highly resistant to antibiotics
Enterobacteriaceae • Sources of infections • Animals, usually through eating contaminated meat • Humans, passed commonly by the fecal oral route • Endogenous spread can occur in some patients where the bacteria spread from intestines to the bloodstream or to the urinary tract • Medical Importance • Most frequent cause of diarrheal disease • 4 billion infections per year • 3 million deaths per year • More morbidity than any other bacterial group
Enterobacteriaceae • Identification of genus and species • Growth on selective-differential media • Selects for Gram-negative bacteria • Differentiates different species by fermentation of sugars and endproducts • Strain Identification (Serotyping) • O Antigen – Lipopolysaccharide (LPS) • K Antigen – Capsule • H Antigen – Flagella
Enterobacteriaceae • Virulence Factors • Endotoxin • Cytotoxic – kills some cells • Inflammation (Lipid A) • Activates complement • Recruitment of white blood cells (WBC) • Fever induction • Release of cytokines (Endotoxin Shock and Death) • Capsule • Protects against phagocytosis and killing by WBC
Enterobacteriaceae • Fimbriae • Attachment to our cells • Antigenic phase variations • Some bacteria can change expression of H antigen (flagella) and K antigen (Capsule) in response to antibodies in environment. Therefore, they stay one step ahead of the immune system • Exotoxins • Very important for diarrheal diseases • But not all enterics produce exotoxins • Now lets look at the species individually
Escherichia coli • E. coli exists in large numbers in GI tract • Most infections spread from within • Most important cause of nosocomial infections • Virulence factors • Fimbriae for adhesion • Exotoxins play important roles in some types of diarrhea caused by this pathogen • Infections are divided into two groups • extra-intestinal • intestinal
Escherichia coli • Extra-intestinal disease • Urinary tract infections (UTI) • 80% of all community-acquired UTIs • 90% of UTIs in women • Local spread from intestinal tract • Septicemia (bloodstream) • Most common cause among hospital patients • Spread from GI tract or UTI • Neonatal meningitis (Brain lining) • Leading cause
Escherichia coli • Intestinal disease (diarrhea) • Enterotoxogenic • Enteroinvasive • Enteropathogenic • Enterohemorrhagic • Enteroaggregative • Differ based upon • Toxin production • Invasion or noninvasive • We will only focus on Enterotoxogenic and Enterohemorrhagic since they are the most well characterized
Escherichia coli • Enterotoxogenic • >50% of travelers diarrhea acquired when we travel to a foreign country • Natives in country have immunity and don’t get sick • However, infants are born without immunity and can get sick even if native of the country and this this type of diarrhea is the #1 cause of infant death in developing countries • We get this type of E. coli from contaminated food and water


![GRAM NEGATIVE BACILLI- MICRO {ST1]](https://cdn1.slideserve.com/2240310/gram-negative-bacilli-micro-st1-dt.jpg)