Download
1 / 29
360 likes | 1.84k Views
Dr KN POORNESH WGH 03.11.2004. RETINAL VEIN OCCLUSION. CLASSIFICATION. BRVO CRVO Major BRVO Non-ischemic Minor Macular BRVO Ischemic Peripheral BRVO Papillophlebitis Hemiretinal Vein occlusion . PATHOGENESIS.

E N D
Dr KN POORNESH WGH 03.11.2004 RETINAL VEIN OCCLUSION
CLASSIFICATION BRVO CRVO Major BRVO Non-ischemic Minor Macular BRVO Ischemic Peripheral BRVO Papillophlebitis Hemiretinal Vein occlusion
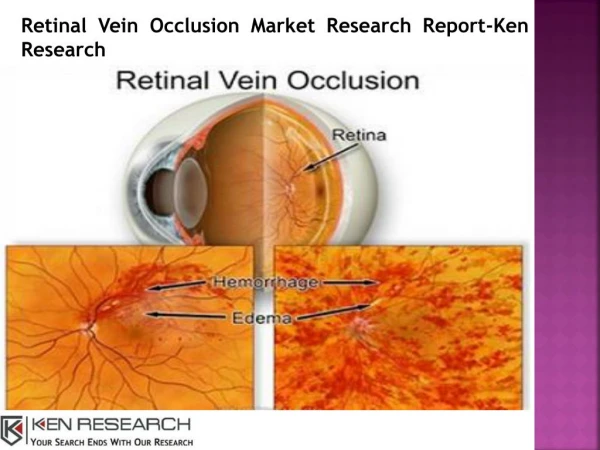
PATHOGENESIS Arteriosclerosis Compression of the vein Venous endothelial cell loss Thrombus formation Venous Occlusion
PATHOGENESIS Venous occlusion elevation of venous & capillary pressure Stagnation of blood flow Increased tissue pressure Hypoxia of the retina Damage to capillary endothelial cells & extravasation of blood constituents
RISK FACTORS(in order of importance) • Advancing age: 50% cases over 65 yrs. • Systemic: HT, Hyperlipidemia, Diabetes, Smoking, Obesity. • Raised IOP: risk of CRVO • Inflammatory: Behcet’s, Sarcoid,AIDS, SLE, Toxoplasma. • Hyperviscosity: Polycythemia, MM, Waldenstrom macroglobulinemia.
RISK FACTORS 6. Acquired thrombophilic: Hyperhomocystinemia, Antiphospholipid antibody syndrome. 7. Inherited thrombophilic: increased levels of clotting factors 7 & 11, deficiency of antithrombin 3, protein C &S, resistance to activated protein C. Other Risk factors: •Hypermetropia (BRVO), Congenital anomaly of Central retinal vein (CRVO), Optic disc drusen, • Drugs (OC, Diuretics), Migraine (rare). • Retrobulbar external compression: Dysthyroid eye disease, Orbital tumor
COURSE of BRVO 6 to 12 months to resolve • Venous sheathing • Collateral venous channels • Microaneurysms, Hard exudates, Cholesterol crystal deposition. • Macula: RPE changes or ER gliosis, chronic CME.
Prognosis and Complications of BRVO Depends on • Site & Size of occluded vein • Integrity of perifoveal capillary network 50% : Recover VA of 6/12 or better. Complications: 1. Chronic macular edema 2. Macular ischemia 3. Neovascularisation, NV (within 3 yrs) 10%- NVD, 20-30%- NVE 4. Recurrent VH, TRD.
Management of BRVO(BVOS) Wait for haemorrhage to clear (3 months). FFA : • Macular edema and VA 6/12 or worse after 3 months –grid laser & follow-up after 2-3 months. • Macular ischemia—no treatment. • 5 DD or > area of CNP– 4 monthly follow- up for 12-24 months. • Neovascularisation– scatter laser
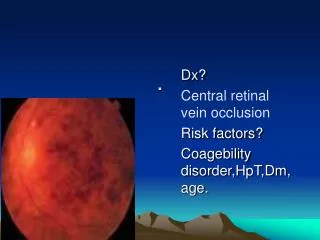
Non-ischemic CRVO(Course and Follow-up) Residual signs: Disc collaterals, epiretinal gliosis, pigmentary changes at macula. Conversion to ischemic CRVO occurs in 15% of cases within 4 months and 34% within 3 years. Follow-up: should be for 3 years. Prognosis: depends on initial VA, near normal VA in 50%, Chronic CMO- unresponsive to laser (CVOS). 8-10% risk of BRVO or CRVO in the fellow eye.
Ischemic CRVO:Management (CVOS) Follow-up: monthly for 6 months IOP, undilated gonioscopy & SLE Angle NV is the best clinical predictor of NVG. Treatment: PRP in eyes with angle or iris NV. Monthly follow-up until stabilisation or regression.
Hemiretinal vein occlusion • Less common than BRVO and CRVO • Occlusion of superior or inferior branch of the CRV. • Features of BRVO, involving the superior or inferior hemisphere • Prognosis depends on severity of macular edema and ischemia.
PAPILLOPHLEBITIS(Optic disc vasculitis) • Healthy individuals, < 50 years • Optic disc swelling with secondary venous congestion rather than venous thrombosis. • APD absent, retinal haemorrhages confined to posterior fundus. • Prognosis: 80% -- 6/12 or better 20% visual loss -- macular edema
Management:Recent advances • Recent onset of non-ischemic CRVO– high intensity laser to create chorioretinal shunt. • AV sheathotomy for treatment of CME due to BRVO. • Ischemic CRVO:- PP Vitrectomy + Intraocular gas + Radial neurotomy
Management: Recent advances • Intravitreal tPA • Transvitreal vein cannulation • Section of posterior scleral ring • Drug therapy -- Troxerutin -- Petroxyfylline -- Hemodilution • Intravitreal Triamcinolone