Download
1 / 2
40 likes | 338 Views
Root canal re-treatment. Should we dismantle? This patient presented complaining of an intermittent throbbing pain in the region of tooth 46. The tooth had been root filled approximately 17 years previously and had only recently become problematic.

E N D
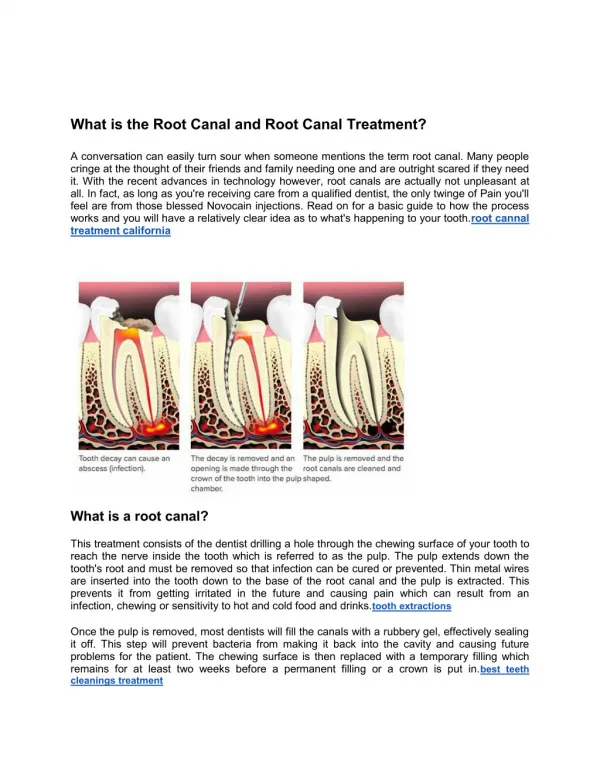
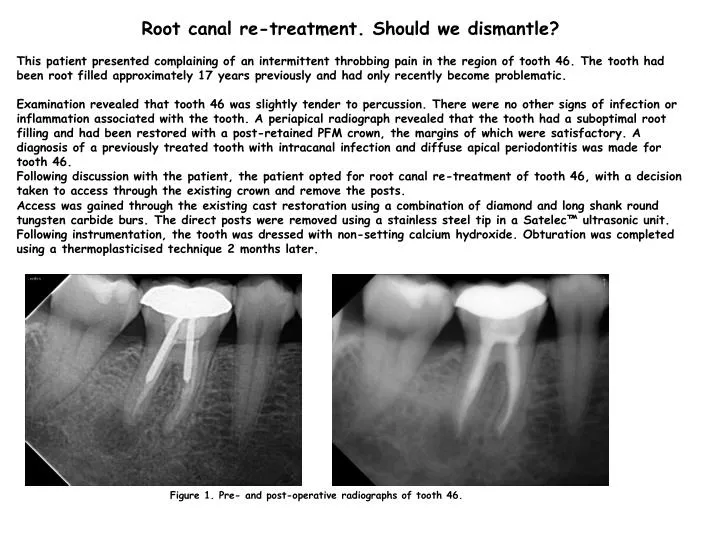
Root canal re-treatment. Should we dismantle? This patient presented complaining of an intermittent throbbing pain in the region of tooth 46. The tooth had been root filled approximately 17 years previously and had only recently become problematic. Examination revealed that tooth 46 was slightly tender to percussion. There were no other signs of infection or inflammation associated with the tooth. A periapical radiograph revealed that the tooth had a suboptimal root filling and had been restored with a post-retained PFM crown, the margins of which were satisfactory. A diagnosis of a previously treated tooth with intracanal infection and diffuse apical periodontitis was made for tooth 46. Following discussion with the patient, the patient opted for root canal re-treatment of tooth 46, with a decision taken to access through the existing crown and remove the posts. Access was gained through the existing cast restoration using a combination of diamond and long shank round tungsten carbide burs. The direct posts were removed using a stainless steel tip in a Satelec™ ultrasonic unit. Following instrumentation, the tooth was dressed with non-setting calcium hydroxide. Obturation was completed using a thermoplasticised technique 2 months later. Figure 1. Pre- and post-operative radiographs of tooth 46.
The patient returned for review six months following completion of treatment. She was asymptomatic and there were no clinical signs of infection or inflammation associated with tooth 46. A periapical radiograph revealed good signs of periapical healing. Figure 2 Six month recall radiograph of tooth 46 showing signs of healing Discussion This case highlights the potential to access through the existing restoration assuming it is satisfactory both clinically and radiographically. This often negates the need to replace the cast restoration following endodontic treatment, at least in the short-term, thereby making it a more financially acceptable solution to the patient. Root canal re-treatment of these teeth requires appropriate magnification and illumination and also the correct armamentarium in order to enhance the possibility of a satisfactory result. Final restoration of the tooth also requires the correct protocol for placement of a composite restoration in an existing crown.