Download
1 / 21
210 likes | 542 Views
肝豆状核变性 Wilson’s Disease. 2009 年 2 月 9 日. 肝豆状核变性(肝豆病) Hepatolenticular degeneration (HLD) Copper storage disease Wilson’s Disease (WD).

E N D
肝豆状核变性Wilson’s Disease 2009年 2月9日
肝豆状核变性(肝豆病) Hepatolenticular degeneration (HLD) Copper storage disease Wilson’s Disease (WD) The disease bears the name of theBritish physician Dr Samuel AlexanderKinnier Wilson (1878-1937), a neurologistwho described the condition in 1912.
概述 • 常染色体 • 隐性遗传 • 铜代谢障碍 游离铜大量沉积 铜排泄障碍 肝脏症状 神经精神症状 肾脏损害症状 • 最基本的遗传缺陷: ATP7B基因突变导致铜蓝蛋白合成障碍 copper-transporting P-type ATPase
1--2 mg /d 铜代谢 Normal absorption and distribution of copper. Cu = copper, CP = ceruloplasmin, green = ATP7B carrying copper CMT1= copper membrane transporter 1 TGN=高尔基体
Cu作为辅酶参与多种生物酶合成发病机理 细胞色素氧化酶 cytochrome oxidase Cu/Zn结合的过氧化物歧化酶 Cu/Zn-binding superoxide dismutase 铜蓝蛋白 Ceruloplasmin mono amino oxidase lysil oxidase tyrosinase
Initially…eventually… ATP7B 缺陷 铜蓝蛋白
发病率约为 1/30万 • 男:女 = 1:4 • 儿童和青少年:肝脏表现,10~13岁高发 • 成人表现为神经系统症状,19~20岁高发 • 进行性肝衰竭、脑病、凝血障碍、死亡(如果不及时肝移植)
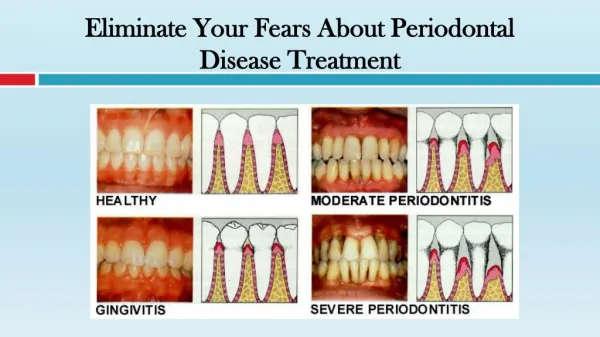
临床表现 大部分肝损害症状隐匿、进展较缓慢,就诊时才发现肝硬化和脾肿大,甚至腹水。 厌食、恶心等消化道症状 黄疸、腹部膨隆 溶血性贫血和血小板减小 肝脏损害: 1.慢性活动性肝炎 2.肝硬化 3.爆发性肝衰竭 小叶性肝硬化,表面有大小不等的结节,光镜示肝细胞严重坏死,肝纤维囊高度细胞浸润;萎缩的肝小叶内结缔组织明显增生,组织化学证明肝组织内不规则岛状分布的铜颗粒沉着
精神症状 -注意力记忆力减退、反应迟钝、情绪不稳、伴傻笑、强笑 -冲动行为、人格改变 -后期明显的痴呆 • 神经症状 -儿童:舞蹈样动作、手足徐动、肌张力不全、小脑共济失调、面部怪容、张口流涎、构音障碍、吞咽困难、上肢扭转动作与快速无目的动作相间,下肢呈跳跃性不规则步态。后期:持久性全身扭转痉挛,痛性发作。 -成人:肌强直、动作减少、慌张步态、震颤
角膜色素环(Kayser-Fleisher环,K-F环)重要体征 肉眼或裂隙灯在角膜后弹力层周边部可见棕色、灰色环。 • Asymptomatic • Golden-brown, orange or grayish ring of copper deposits at the level of Descemet's membrane • Located in corneal periphery, which initially appears as thin crescent deposits at 12 to 6 o'clock and may eventually form a complete ring • May regress or disappear when the systemic condition is well treated
其他表现 Hematological 急性非免疫性溶血性贫血 鼻衄 由于红细胞内 高浓度的铜导致 氧化损伤进而发 生血管内溶血。 Orthopedic 软骨钙质沉着 代谢性骨病 青少年多发关节炎 经常性骨折或脱位 由于钙磷代谢障碍 Renal 氨基酸尿 高钙尿 镜下血尿 蛋白尿 肾性糖尿 Skin 色素沉着 (类似 Addison's disease) 面部和双小腿伸侧明显 铜沉积 Cardiovascular 心律失常 类似于风湿性发热的表现 Gynecological 原发或继发性闭经 反复的或不明原因的流产 Ocular Sunflower cataract (葵花状内障)
Complications • Hepatitis • Cirrhosis • Death of liver tissues • Spleen dysfunction • Anemia • Increased number of infections • Injury caused by falls • Loss of ability to interact with other people • Loss of ability to function at work and home • Loss of ability to care for self • Loss of muscle mass (muscle atrophy) • Joint contractures or other deformity • Increased number of bone fractures • Side effects of penicillamine • Side effects of other medications used to treat the disorder
鉴别诊断 Wilson's disease: an update Shyamal K Das and Kunal Ray Nature Clinical Practice Neurology (2006) 2, 482-493 铜代谢检查K-F环
实验室检查 • 铜代谢方面的主要检查: 血清铜<正常值50% (17.4~20.5 umol/L) 血清铜蓝蛋白<0.2g/L (0.26~0.36g/L) 24小时尿铜>1.6umol/24h (<0.24~0.48umol/24h) • 肝肾功能: PT and PTT 、AST and ALT、胆红素、BUN、CREA 血清总蛋白、血尿酸 • 影像学:双侧豆状核区 • 基因诊断: 限制性片段长度多态性分析 微卫星标记分析 半巢式PCR-酶切分析 荧光PCR • 其他 溶血性贫血、WBC计数减少
治疗 • reduce the amount of copper in the tissues • manage the symptoms of the disorder • lifelong 1. 限铜:坚果类、巧克力、豌豆、蚕豆、玉米、蘑菇、贝类、螺类、虾、鱿鱼、动物肝和血; 2.药物(见下表) 3.对症:保肝、抗精神病 4. 脾切除、肝移植
Anti-copper drugs used in the treatment of Wilson's disease.
小结 • Wilson氏病是一种常染色体隐性遗传铜代谢障碍病; • 特征为过量的铜沉积在肝、脑和其他组织; • ATP7B基因的染色体13q区突变影响铜转运ATP酶功能进而使铜蓝蛋白合成障碍; • 常表现为肝脏症状和神经系统症状; • 主要诊断依据为:K-F环、血清铜、血清铜蓝蛋白、24小时尿铜
麻醉注意 • 多器官损害--贫血、低蛋白血症和血凝障碍程度有所减轻后再行手术 • 不加重脏器功能损害和维护生理功能--尽可能应用局麻或神经阻滞麻醉 • 腹部手术则以硬脊膜外麻醉为首选, 平面控制在T5以下, 术中适量的辅助药, 保证供氧和避免二氧化碳蓄积 • 例如有构语障碍、咽喉反射迟钝等症状者,加强术中管理,术中不适、多不能主动诉述或配合, 应及早处理若有呕吐应及时清除, 避免误吸。 • 此类病人的药物消除半衰期延长, 排泄缓慢,故麻醉用药量要减少, 应避免使用可能有损肝肾功能的药物(如氟烷), • 易引起椎体外系症状的药物(如氟哌啶), 应予减量 • 由于肝功能不全, 脾功能亢进,凝血因子合成减少, 血小板破坏增加, 术中渗血较多,应给予止血药一氨基己酸对“ 肝豆”病人出血倾向治疗效果较好 • 同时及时补充血容量, 维持循环功能稳定。
more sensitive to neuromuscular relaxants than normal patients by virtue of reduced muscle function resulting either from the disease itself or from the use of Dpenicillamine. • Some researchers have observed that visual and auditory evoked potentials are altered in WD patients, suggesting damage of the encephalic structures and cerebral trunk. However, the peripheral nerve condution and the somatic-sensory evoked potentials are normal. Such evidence suggests that the regional administration of local anesthetics to WD patients may be safe, since the peripheral nerve transmission is not altered.