Download
1 / 90
1.05k likes | 1.72k Views
D-TGA. Dr. Tahsin.N. TRANSPOSITION. Abnormal origin of the Aorta and Pulmonary Artery from the ventricular complex Atrioventricular concordance with ventriculo -arterial discordance Abnormal spatial relationship of the great arteries Results in two circulations in parallel.

E N D
D-TGA Dr. Tahsin.N
TRANSPOSITION • Abnormal origin of the Aorta and Pulmonary Artery from the ventricular complex • Atrioventricular concordance with ventriculo-arterial discordance • Abnormal spatial relationship of the great arteries • Results in two circulations in parallel
Incidence & Prevalence • 5% to 7% of all congenital cardiac malformations • The incidence is reported to range from 20.1 to 30.5/100,000 live births • strong (60%–70%) male preponderance
Embryology 1. Spiral aortico-pulmonary septum forms but does not spiral or twist during its partitioning of the truncusarteriosus a. Aorta arises from right ventricle b. Pulmonary trunk arises from the left ventricle 2. Result is two closed circuits a. Systemic – unoxygenated – repeatedly re-circulated b. Pulmonary - oxygenated - repeatedly re-circulated
Embryology • The normal conus is subpulmonary, left-sided and anterior ; it prevents fibrous continuity between the pulmonary and tricuspid valve rings. • In TGA, the infundibulum is usually subaortic, right-sided and anterior; it prevents fibrous continuity between the aortic and tricuspid valve rings and further results in abnormal pulmonary to mitral valve ring fibrous continuity.
Anatomy • The common clinical type - situssolitus of the atria, concordant AV and discordant ventriculoarterialalignments - complete TGA. • TGA {S,D,D} - TGA with situssolitus (S) of the atria and viscera, usual (D) looping of the ventricles and an anterior and rightward (D) aorta.
Anatomy- Great artery relationship • Situssolitus and intact ventricular septum - the aortic root is directly anterior or anterior and to the right of the pulmonary trunk in a slightly oblique relationship • Less commonly, the aorta may be positioned anterior and to the left or, rarely, posterior and to the right of the pulmonary trunk.
Coronary Anatomy • The two aortic sinuses of Valsalva adjacent to the aorticopulmonary septum that “face” the pulmonary artery contain the ostia of the coronary arteries in more than 99% of cases
Coronary anatomy • Usual-66.9 • CX from RCA-16.1 • Single RCA-3.9 • Single LCA-1.7 • Inverted-2.4 • Intramural LCA-2.1 • Other-1.6
SA node artery • Origin and proximal course of artery may be variable;reaches the sinus node by the interatrial groove on the anterior surface of the heart, occasionally with an intramyocardial course in the anterosuperior rim of the fossaovalis. • It can be damaged easily during balloon atrialseptostomy, during surgical septectomyor when this portion of the septum is widely excised as in the Mustard or Senningatrial switch operation.
Anatomy - Coexisting Anomalies • Nearly half of the hearts have no other anomaly except a PFOor a PDA. • The VSD is the most frequent coexisting anomaly-40% to 45%. - perimembranous (conoventricular33%) - AV canal (inlet septum 5%) - muscular (27%) - malalignment (30%) - conalseptalhypoplasia type (5%)
VSD • The subaorticstenosis caused by the anterior malalignment of the infundibular septum is frequently associated with aortic arch hypoplasia, coarctation or even complete interruption of the aortic arch • Posterior (leftward) malalignment is associated with varying degrees of LVOTO–subpulmonarystenosis, annular hypoplasia or even pulmonary valvaratresia
SubpulmonaryStenosis 25% [5%] • Fixed -Circumferrential fibrous membrane /diaphragm - Fibromuscular ridge - Herniating tricuspid leaflet tissue - Anomalous MV septal attachments - Tissue tags from membranous septum • Dynamic-associated with SAM
Subaortic Obstruction • Rightward and anterior displacement of the infundibular septum • Associated aortic arch anomalies - hypoplasia - coarctation - interruption Asso. RV hypoplasia & tricuspid valve anomalies
TV anomalies Nearly 31% Functionally imp 4% Ratio of tricuspid to mitral anulus circumference is less than 1 in almost 50% of cases, whereas in normal hearts this ratio is always greater than 1
TV anomalies • Straddling/overriding of chordae • Overriding of the tricuspid annulus • Abnormal chordalatatchments • Dysplasia • Accessory tissue • Double orifice
MV anomalies Nearly 20% Functionally imp 4% • Cleft anterior mitral valve leaflet • anomalous papillary muscles and chordae • Straddling • redundant tissue tags
Juxtaposition of atrial appendages • Both appendages or left + part of right are adjacent • 2-6% • Left > right -6x • Female preponderance • often additionally associated with major cardiac pathology, including dextrocardia, VSD, bilateral infundibulum, right ventricular hypoplasiaand tricuspid stenosis or atresia. • Imp in BAS
Bronchopulmonary Collateral Circulation • Bronchopulmonaryanastomotic channels > 30% of infants with TGA under 2 years of age • Persistence of a significant bronchopulmonary collateral circulation after surgical repair - large enough left-to-right shunt – CCF - warrant catheter embolization
PBF • 50% of the patients - greater proportion of blood flow to the right lung than normal due to rightward alignment of MPA • associated with some degree of hypoplasia of the left pulmonary arterial vessels and is further manifested in the occasional reports of unilateral, always left-sided, pulmonary vein stenosis or hypoplasia.
Determinants of effective gas exchange • Effective ventilation • Effective Pulmonary circulation • Pulmonary blood flow • Pulmonary vascular resistance • Existence of a communication between pulmonary and systemic circuits • Persistent fetal channel – PFO or DA • Abnormal channels – ASD, VSD • Effective delivery of oxygenated blood to the tissues
Definition of shunts • Anatomical shunts • Left to Right: Blood flowing from left sided chambers to the right sided chambers • Right to Left: Blood flowing from right sided chambers to the left sided chambers
Definition of shunts • Physiological shunts • Left to right: The volume of oxygenated pulmonary venous return recirculated to pulmonary circulation (Qp – Qep) • Right to left shunt: The volume of systemic venous return that contributes to cardiac output (reentering the systemic circulation) without having passed through the pulmonary circulation (Qs – Qep)
Definition of shunts • Effective pulmonary blood flow (Qep): • The volume of systemic venous return that is effectively oxygenated in the lungs • Effective systemic blood flow (Qes): • The volume of oxygenated pulmonary venous return that enters the systemic circulation and perfuses the systemic capillary bed
TGA: Atrial and Ventricular level shunts = Effective Systemic Blood Flow • From LA to RA / LV to RV • Anatomically left to right • Physiologically, this volume of oxygenated blood enters systemic circulation. Hence, they contribute to Qes
TGA: Atrial and Ventricular level shunts = Effective PBF • From RA to LA/ RV to LV • Anatomically, right to left shunt • Physiologically, this volume of systemic venous blood enters pulmonary circulation. Hence they contribute to Qep
Recirculating Oxy Blood Recirculating systemic blood
TGA: Shunt at PDA level • Aorta to PA flow: • Anatomically it is left to right • Here the deoxygenated systemic venous blood enters pulmonary circulation. Hence, this volume contributes to Qep • PA to Aorta flow: • Anatomically it is right to left • Here the oxygenated blood enters systemic circulation. Hence, this volume contributes to Qes • Thus, the flow across the ductus is functionally opposite to that of flow across ASD or VSD in TGA
Systemic venous return Pulmonary venous return Anat R-L Anat L-R RIGHT HEART LEFT HEART Physio R-L Physio L-R LUNGS BODY
Unique feature • Net inter-circulatory mixing volume is constant: net R-L, L-R, Qep and Qes are equal to each other • Any major difference in the volumes would result in depletion of blood volume of one circulation at the expense of overloading the other circulation
Precise factors controlling intercirculatory exchange SPECULATIVE, MULTIPLE • LOCAL PRESSURE GRADIENTS • Compliance of the cardiac chambers • Phase of respiratory cycle • Vascular resistances • Heart rate • Volume of blood flow
Flow across the communications“Rules of the Heart” • With only ASD, the flow has to be bidirectional • If the flow is only or predominantly left to right across the ASD, it suggests presence of additional shunt (VSD or PDA) • Unrestrictive VSD - flow is bidirectional • Except in the initial few days, PDA flow is always left to right (Ao to PA). • Presence of right to left flow across ductus may suggest the presence of coarctation of aorta
Right to Left Shunt Systole VSD Left to Right Shunt Diastole
Initially, bidirectional flow across the ductus • Later, once the PVR falls, the flow essentially becomes aorta to PA • The pulmonary circulation becomes overloaded fast, especially if the PFO is restrictive PDA
Factors influencing systemic saturation • Extent of inter-circulatory mixing and Total pulmonary blood flow • High PBF results in increased oxygenated blood available in the left sided chambers for mixing: higher systemic SO2 if there is good mixing • Reduced PBF will result in low systemic SO2 in spite of adequate anatomic shunts
Factors influencing systemic saturation • If there is delay in the fall of PVR (PPHN), hypoxemia will persist despite adequate ASD • Need ECMO or urgent ASO • Hypoxemia provokes a fall in SVR and increase the recirculating systemic volume • Fall in SVR may deplete the pulmonary circulation further
Role of bronchopulmonary collaterals • Systemic arterial hypoxemia may stimulate development of bronchpulmonarycollaterals • Usually in TGA with solely a restrictive inter-atrial communication • Prolonged survival of such infants may be due to this extra-cardiac site of shunting/mixing
History • M:F – 4:1;unless juxtaposition of atrial appendages • Usually in multigravida-2X increase in > 3 pregnancies • Familial recurrence-monogenic inheritance
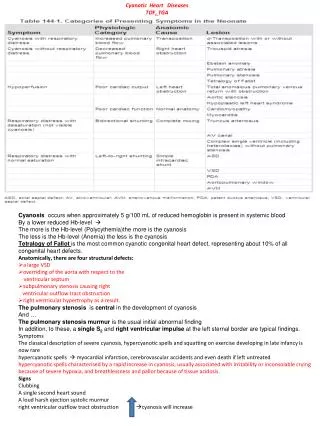
Cyanosis • As early as day 1 in pts with IVS(1st hr-56%;1st day-90%) • More intense if associated PS/atresia • Mild if associated non restrictive VSD • PS often responsible for hypercyanotic spells-intense cyanosis, tachypnea, extreme irritability and hypothermia • Squatting is rare • Reverse differrential cyanosis
CHF • In patients with a large PDA • Large VSD
Mortality • 1st week-30% • 1st month-50% • 1st year-90% • Depends on the degree of shunting • Moderate PS improves survival • Predilection for brain abscess but rare < 2 years
Appearance • Birth weight greater than normal • Reverse differential cyanosis • Varicosities of scalp and arms
Arterial Pulse • Bounding pulse - due to large volume of highly unsaturated blood - Not due to PDA-since only systolic shunt from aorta to PA • Diminished femoral pulses - CoA - Subaorticstenosis-anterior and rightward displacement of septum
Palpation • Nomal in neonates • RV impulse in patients with CHF • LV impulse – non restrictive VSD with low PVR • Palpable S2 A2
Auscultation • Loud A2 • LV S3-mildly cyanosed patients,increased PBF,LV failure • RV S3-deeply cyanosed patients, increased systemic flow, RV failure
Auscultation • Ejection click-pulmonary;doesnot decrease with inspiration • Aortic-subaorticstenosisdilated aortic root • MSM-aortic:hypervolemic and hyperkinetic circulation • Pulmonary: valvular- after few weeks of birth, progressively increases • Subvalvar dynamic obstruction-3rd LICS and radiates to the right
Auscultation • VSD: absentholosystolicshortensabolished • PDA: Systolic if large PDA since high PVR curtails diastolic flow Continuous if restrictive PDA • Continuous murmurs may arise in large systemic arterial collaterals but rare • MDM may be heard across AV valves