Download
1 / 60
660 likes | 1.18k Views
Clinical presentations and pathology of stroke. น.พ. พรชัย สถิรปัญญา สาขาประสาทวิทยา ภาควิชาอายุรศาสตร์ คณะแพทยศาสตร์ ม.สงขลานครินทร์. ประชุมวิชาการชมรมประสาทวิทยาศาสตร์ภาคใต้ ครั้งที่ 7 โรงแรมวัฒนาพาร์ค จ. ตรัง 07/12/2550. Stroke is an emergency !. หัว สมอง. โรคหลอดเลือด. หัวใจ.

E N D
Clinical presentations and pathology of stroke น.พ. พรชัย สถิรปัญญา สาขาประสาทวิทยา ภาควิชาอายุรศาสตร์ คณะแพทยศาสตร์ ม.สงขลานครินทร์ ประชุมวิชาการชมรมประสาทวิทยาศาสตร์ภาคใต้ ครั้งที่ 7 โรงแรมวัฒนาพาร์ค จ. ตรัง 07/12/2550
หัวสมอง โรคหลอดเลือด หัวใจ หัวแม่เท้า
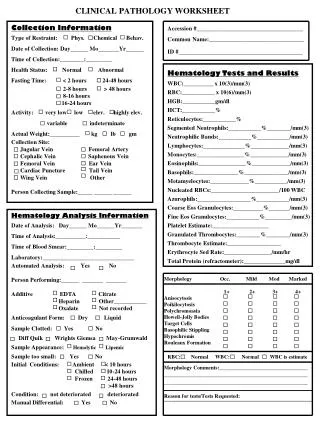
Cerebrovascular disease (CVD) or Stroke • Definition:Arupt focal or global neurological dysfunction lasting more than 24 hrs, leading to death, caused by no other causesthan cerebrovascular in origin.
How to diagnose stroke • Clinical presentations • Neuro-radiological studies -imaging : anatomical and physiological -ultrasonology • Genetic study eg, CADASIL • Pathological studies
“ stroke” • Stroke by clinical diagnosis requires : -Risk factors of cardiovascular diseases -Sudden onset of neurological deficit -The deficit is explainable by neurovascular syndrome *Exclusion of other causes !?
Non stroke • Tumor • Focal infection • Demyelination Arupt neurological deficit 95 % 5%
Anatomical Dx • Supratentorium • (carotid system) • Infratentorium • (vertebre-basilar • system)
Stroke classification (anatomy) • Carotid system stroke : - hemipaparesis and facial palsy UMN - aphasia or other cortical dysfunctions • Vertebrobasilar system stroke - hemiparesis and contralateral facial palsy LMN (or other Cranial n. palsy) - cerebellar and brain stem disorders
ลานฝั่งนที อ.เมือง สงขลา สงขลาฝั่งนที กลิ่นสารภียังติดเตือน...........
Stroke classification Pathological: arterial • Ischemic stroke (C.infarction) 85% - Thrombotic stroke Large vs. small vss. disease - Embolic stroke • Hemorrhagic stroke (C. hemorrhage) 15% - Intracerebral hemorrhage - Subarachnoid hemorrhage - Intraventricular hemorrhage
Thrombotic stroke Embolic stroke
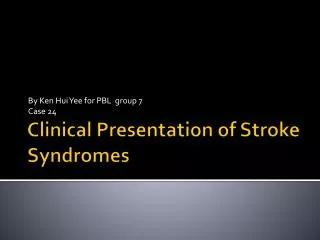
Brain computed tomography showing extensive intracerebral hemorrhage inthe right hemisphere, involvingbasal ganglia and thalamus,with intraventricular hemorrhage. CT head scan showing right intracerebral hemorrhage secondary to ruptured right middle cerebral aneurysm
1 2 Image 1. This is a brain CAT scan image. The yellow arrows point to two aneurysms. Image 2. This is also a brain CAT scan image. The yellow arrow points to a ruptured giant brain aneurysm with some clot (thrombus) within the main aneurysmal sac. The green arrow heads point to blood in the subarachnoid space. This image therefore shows aneurysmal subarachnoid hemorrhage (SAH).
3 4 Image 3. This is a brain magnetic resonance angiogram (MRA). The image is a "scout" image of the Circle of Willis at the base of the brain. The yellow arrows point to six different brain aneurysms. Image 4. show multiple brain aneurysms (yellow arrows). One of the aneurysms has an irregular "daughter sac" (DS) coming off its dome.
Stroke classification • Pathological: venous -Cerebral dural sinus thrombosis -Cerebral cortical v. thrombosis -Internal cerebral v. thrombosis
Risk factors • Modifiable risk factors • Potentially modifiable risk factors • Non-modifiable risk factors
Well-documented risk factors • Modifiable, value established • -Hypertension • most significant modifiable risk factor • Relative risk x 4
. Overall relative risk of total stroke according to approximate usual diastolic blood pressure 18 studies, 1798 events in 124774 participants Lancet 1998;352: 1801-1807
Modifiable, value established • - Cardiac disease • Atrial fibrillation • Infective endocarditis • Mitral stenosis • Recent large myocardial infarction
Modifiable, value established - Cigarette smoking - Sickle cell disease - Transient ischemic attacks - carotid stenosis
Potentially modifiable -Diabetes mellitus -Hyper- homocysteinemia -Left ventricular hypertrophy
Nonmodifiable Age Gender Hereditary/familial factors Race/ethnicity Geographic location
Less well-documented risk factors - Elevated blood cholesterol and lipids - Cardiac disease Cardiomyopathy Patent foramen ovale Atrial septal aneurysm Aortic stenosis Mitral valve prolapse
Overall relative risk of haemorrhagic and non-haemorrhagic stroke, according to approximate usual cholesterol concentration Lancet 1998;352: 1801-1807
- Use of oral contraceptives - Consumption of alcohol - Use of illicit drugs - Physical inactivity
Neuro-radiological studies (anatomical scan)