Download
1 / 18
290 likes | 892 Views
Adenoviruses. By Lesley Aigboboh. Table Of Contents. Introduction Replicative cycle Transmission and Epidemiology Pathogenesis and Immunity Clinical findings Lab diagnosis Treatment and Prevention. Introduction.

E N D
Adenoviruses By Lesley Aigboboh
Table Of Contents • Introduction • Replicative cycle • Transmission and Epidemiology • Pathogenesis and Immunity • Clinical findings • Lab diagnosis • Treatment and Prevention
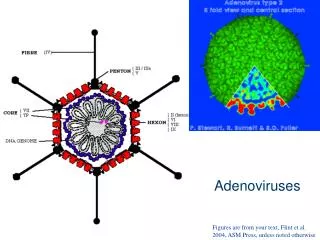
Introduction • Adenoviruses (members of the familyAdenoviridae) are medium-sized (90–100 nm), no non-eneveloped(without an outer lipid bilayer) viruses with an icosahedralnucleo- capsid containing a double stranded DNA genome.
Replicative Cycle • Adenoviruses possess a linear dsDNA genome and are able to replicate in the nucleus of vertebrate cells using the host’s replication machinery. • Entry of adenoviruses into the host cell involves two sets of interactions between the virus and the host cell. Most of the action occurs at the vertices. Entry into the host cell is initiated by the knob domain of the fiber protein binding to the cell receptor. The two currently established receptors are: CD46 for the group B human adenovirus serotypes and the coxsackievirusadenovirusreceptor (CAR) for all other serotypes. There are some reports suggesting MHC molecules and sialic acid residues functioning in this capacity.
This is followed by a secondary interaction, where a motif in the penton base protein interacts with an integrin molecule. It is the co-receptor interaction that stimulates entry of the adenovirus. This co-receptor molecule is αvintegrin. Binding to αvintegrin results in endocytosis of the virus particle via clathrin-coated pits. Attachment to αvintegrin stimulates cell signaling and thus induces actin polymerization resulting in entry of the virion into the host cell within an endosome. Once the virus has successfully gained entry into the host cell, the endosome acidifies, which alters virus topology by causing capsid components to disband. These changes as well as the toxic nature of the pentons result in the movement of the virion into the cytoplasm. With the help of cellular microtubules, the virus is transported to the nuclear pore complex, whereby the adenovirus particle disassembles.
Viral DNA is subsequently released, which can enter the nucleus via the nuclear pore .After this the DNA associates with histonemolecules. Thus, viral gene expression can occur and new virus particles can be generated. The adenovirus life cycle is separated by the DNA replication process into two phases: an early and a late phase. In both phases, a primary transcript that is alternatively spliced to generate monocistronic mRNAs compatible with the host’s ribosome is generated, allowing for the products to be translated.
Transmission and Epidemiology • Adenoviruses are unusually stable to chemical or physical agents and adverse pH conditions, allowing for prolonged survival outside of the body and water. Adenoviruses are spread primarily via respiratory droplets, however they can also be spread by fecal routes. • Humans: Humans infected with adenoviruses display a wide range of responses, from no symptoms at all to the severe infections typical of Adenovirus serotype 14. • Animals: Two types of canine adenoviruses are well known, type 1 and 2. Type 1 causes infectious canine hepatitis, a potentially fatal disease involving vasculitis and hepatitis. Type 1 infection can also cause respiratory and eye infections
Transmission and Epidemiology • Adenovirus in Reptiles is poorly understood, but research is currently in progress. • Adenoviruses are also known to cause respiratory infections in horses, cattle, pigs, sheep, and goats. Equine adenovirus 1 can also cause fatal disease in immunocompromised Arabian foals, involving pneumonia and destruction of pancreatic and salivary glandtissue. Tupaia adenovirus (TAV) (Tree shrew adenovirus 1) has been isolated from tree shrews.
Pathogenesis and Immunity • Certain adenovirus serotypes are associated with distinct clinical manifestations, but the basis for these differences is not well understood. As an example, the group C types 1, 2, and 5 are associated with respiratory tract infections; the group B types 11, 34, and 35 cause hemorrhagic cystitis; and the group D types 8, 19, and 37 are the major causes of epidemic keratoconjunctivitis. Serotype-specific clinical manifestations may be partially determined by differences in cell tropism. Some serotypes, for example, display different cell receptor preferences, which are mediated by the viral attachment protein fiber.
Pathogenesis and Immunity • Although most adenoviruses from groups A, C, D, E, and F bind to the coxsackievirus-adenovirus receptor (CAR), the group B adenoviruses do not bind to this receptor . Group B adenoviruses have been shown to bind to the complement-related protein CD46, as well as CD80 and CD86 (activation markers on hematopoietic cells) . • Adenoviruses elicit both innate and adaptive immune responses. Recovery from adenovirus infection is associated with the development of serotype-specific neutralizing antibodies directed mainly at the major capsid protein hexon
Immunity • The most important host defense against many viruses, including adenoviruses, is cell-mediated immunity. Fatal adenovirus infections occur most commonly in immunocompromised patients, especially those with defects in cell-mediated immunity. Adenovirus-specific memory CD4+ T cells can be detected in most healthy adults and can exhibit cross-reactivity against different serotypes.
Clinical Findings • Adenoviruses most commonly cause respiratory illness; however, depending on the infecting serotype, they may also cause various other illnesses, such as gastroenteritis, conjunctivitis, cystitis, and rash illness. Symptoms of respiratory illness caused by adenovirus infection range from the common cold syndrome to pneumonia, croup, and bronchitis.
Respiratory Diseases • The most important etiological association of adenoviruses is with the respiratory diseases. • They are responsible for 5% of acute respiratory diseases in: • young children • and much less in adults.Also, Epidemic Keratoconjuctivisoccuring with serious epidemic. Occurs with serotypes 8 and less frequently 19 and 37.
Lab Diagnosis Direct detection: • Virus particle byEM can be detected by direct examination of fecal extracts • Detection of adenoviral antigens byELISA. Enteric Adenoviruses • Detection of adenoviral NA by Polymerase chain reaction: can be used for diagnosis of Adenovirus infections in tissue samples or body fluids.
Treatment • There are no antiviral drugs to treat adenoviral infections, so treatment is largely directed at the symptoms (such as acetaminophen for fever). A doctor may give antibiotic eyedrops for conjunctivitis, since it takes a while to test to see if the eye infection is bacterial or viral and to help prevent secondary bacterial infections. Currently, there is no adenovirus vaccine available to the general public, but a vaccine is available for the United States military for Types 4 and Type 7.
Prevention and Control • Careful hand washing is the easiest way to prevent infection. • Disinfection of Environmental surfaces with hypochlorite's. • The risk of water borne outbreaks of conjunctivitis can be minimized by chlorination of swimming pools. • Epidemic keratoconjunctivitis can be controlled by strict asepsis during eye examination.
References • Goldstein, T.; Colegrove, K. M.; Hanson, M.; Gulland, F. M. D. (2011). "Isolation of a novel adenovirus from California sea lions Zalophuscalifornianus. • "Isolation and identification of a fowl adenovirus from wild Black Kites (Milvusmigrans)". Journal of wildlife diseases • Naskalska, A.; Szolajska, E.; Chaperot, L.; Angel, J.; Plumas, J.; Chroboczek, J. (2009). "Influenza recombinant vaccine: Matrix protein M1 on the platform of the adenovirus dodecahedron“.