Download
1 / 25
300 likes | 1.68k Views
FOURTH NERVE / SUPERIOR OBLIQUE PALSY FNP / SOP. LIONEL KOWAL RVEEH / CERA MELBOURNE. Types of apparent FNP / SOP All of these LOOK THE SAME. 1. Definite SOP Only true HALF the time that it is diagnosed! 2. Possible SOP or Resolved SOP 3. Idiopathic oblique dysfunction & other

E N D
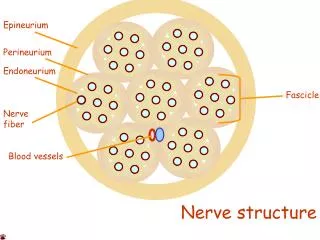
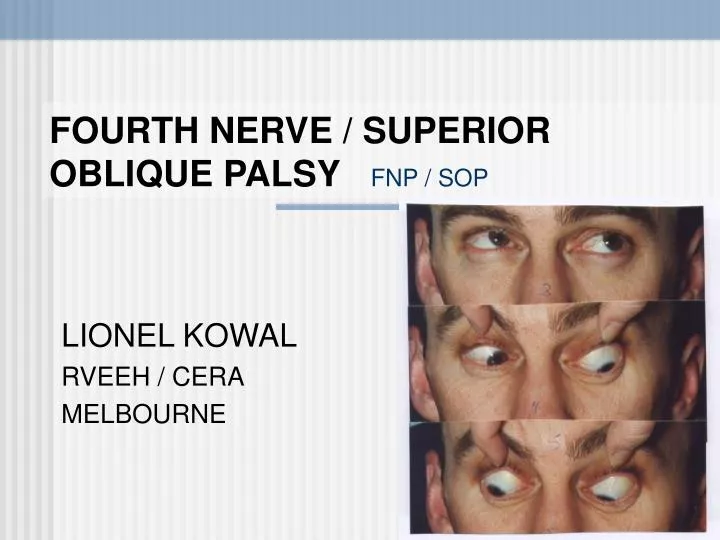
FOURTH NERVE / SUPERIOR OBLIQUE PALSYFNP / SOP LIONEL KOWAL RVEEH / CERA MELBOURNE
Types of apparent FNP / SOPAll of these LOOK THE SAME • 1. Definite SOP Only true HALF the time that it is diagnosed! • 2. Possible SOP or Resolved SOP • 3. Idiopathic oblique dysfunction & other synonyms for …“CycloVertical Dysfunction of uncertain cause” = CVD Mostly due to minor anatomical ‘errors’ • 4.Pulley heterotopy radiological diagnosis • 5. Something quite different Graves’, old fracture, other vertical rectus disease, post ret-det surgery, …
Definite SOP / Possible SOP / CVD / pulley heterotopy ….. can all • Vertical misalignment • Disrupt horizontal fusion & horizontal misalignment • Head tilts • Vertical greater to one side • Apparent IO OA, SO UA CLINICAL PICTURE CAN BE THE SAME IN ALL THESE TYPES OF SOP & PSEUDO - SOP
Is it important to differentiate? LUMPERS Traditional UK approach All SOPs get similar treatment • Lumpers vs splitters SPLITTERS Post 1950’s US approach Individualise treatment to specific subtype of SOP
Lumpers • If it looks / smells / sounds … a bit like SOP, then call it SOP. • ‘Congenital SOP’ label used with NO evidence of true palsy • Rx: inf obl weakening IO- Some lumpers: one size fits all. Some : 2-3 different ops • Nucci: Milan, EJO sectional editor, trained Italy & Chicago, 62 articles in PubMed,…
Splitters • Knapp: important to split 7 different types based on detailed measurements and versions Later subclassified further by others • some pts do well with IO- • others will do better with SO plication or SR weakening…… • Selection bias: strabismus specialist tends to see pts with inadequate results after IO- • LK: a splitter
Lumpers vs Splitters & EBM 21st Century: issues resolved by randomised prospective trial - still waiting Eminence based medicine Loudest most forceful & charismatic medical conference personality defines clinical practice. MOST strabismus specialists are splitters
Splitting…… • 1. Careful measurements in cardinal positions Allows classification into Knapp types [or more modern variants] and likely surgical solution
Splitting…… • 2. Radiology: Is it a True SO atrophy: More likely to have floppy SO ?less likely to respond to IO- ?more likely to need SO+
When strabismus specialists made clinical diagnosis of SOP, they were wrong 50% of the time!! MRI X-sectional area of SO segregates SOP from normal SO
Splitting…… 3. Reserve final surgical plan until intra-operative FDT If SR is tight, more likely to need SR- If SO floppy,…. If IO is tight,… If IR is tight,… Need a MUCH larger surgical repertoire than Lumpers
R SOP HEAD TILT TO LEFT
ADAPTATION TO WEAK SO R IO OA ADAPTATIONS MAY DOMINATE THE CLINICAL PICTURE CORE DEFECT R SO UA ADAPTATION TO CHRONIC HYPERTROPIA TIGHT RSR RIR ‘UA’
SOP image LSO OK RSO ?absent
Case #1 • Atrophic SO • SO UA • IO OA SOUA > IO OA • IR UA [presumed tight SR from having had a ‘chronic hypertropia’] • LUMPERS : Inf obl weakening • SPLITTERS : Final decision after FDT
Splitters • Atrophic SO and SO UA: More likely to find floppy SO More likely to need SO plication • Apparent IR UA Probably tight SR Needs SR- or will have DG diplopia • If FDT on SO & SR are OK: IO-
Principles of treatment Acquired SOP : 12 mo [can Rx earlier if getting worse] Long standing: Acquired suppression makes it harder to characterise SPLITTERS: Usually have to treat the muscular consequences of the SOP rather than the SOP itself
Principles of treatment • Make it better - don’t over correct • Trauma: look for bilateral SOP • Accurate measurements SPLITTERS • Tighten floppy muscles • Recess tight muscles
Principles of treatment : IO- Parks’ IO Rc for 10-15 ∆ height in PP ≈ 20 ∆ To lateral edge IR ≈ 25 ∆ 2mm ant to edge IR
Principles of treatmentTight SR ‘Chronic hypertropia’ may tight SR, spread of comitance & [apparent] IR UA wch may come to dominate the clinical picture. SR Rc required Recessing SR will increase extorsion unless it is temporally transposed
TREATMENT EXPECTATIONS • LK audit early 90’s n=450 • Unilateral SOP [all sorts]: • 1.3 surgeries • 90+% Very Good to excellent
SOP • Difficult area of strabismus • Lumpers vs Splitters : unresolved • Splitters more likely to see the more complex pts & believe that a more complicated approach is the correct one
The contralateral inferior rectus Lumpers • 1st op: inf obl • 2nd op: c/l inf rectus Splitters • Consider c/l inf rectus if tight or if SO UA without SO floppiness
The contralateral inferior rectus • MRI of the Functional Anatomy of the Inferior Rectus Muscle in Superior Oblique Muscle Palsy.Jiang L, Demer JL.UCLA Ophthalmology. November 2008. • PURPOSE: Biomechanical modeling consistently indicates that SO muscle weakness alone is insufficient to explain the large hypertropia often observed in SOP. MRI : to investigate if any size or contractility changes in IR may contribute. • 17 pats with unilateral SOP and 18 orthotropic controls. • Diagnosis of SOP based on clinical presentations, subnormal contractility & small SO muscle size
The contralateral inferior rectus • OUTCOME MEASURES: X-sectional areas of IR & SO. • RESULTS: Patients had 16+/-7∆ of central gaze hypertropia and exhibited ipsilesional SO muscle atrophy and subnormal contractility. • CONCLUSIONS: ..the contralesional IR is larger and more contractile than the ipsilesional IR, reflecting likely neurally mediated changes that augment the relatively small hypertropia resulting from SOP. • Recession of the hyperfunctioning contralesional IR in SOP is a physiologic therapy.