Download

1 / 51
• 510 likes • 525 Views
Learn about the importance of glucose monitoring, different monitoring methods, and the future of diabetes technology. Understand the limitations and common errors of self-monitoring of blood glucose (SMBG) and how to overcome them.

E N D
Glucose Monitoring Dr. Kashi Professor of endocrinology Diabetes research center Mazandaran university of medical sciences Dr.Sarma@works
case • A 49-year-old, African-American man, a computer engineer • his clinician tells him that his diabetes is uncontrolled, but the patient is sure that it is well controlled. • Five years ago, he developed polyuria, polydipsia, nocturia, and lost 23 lbs over a four-month period. A random blood glucose level was 277 mg/dL .The glycated hemoglobin (A1C) was 10.8 percent. The patient was treated with medical nutrition therapy and metformin 1000 mg twice a day with meals. • The patient adhered to his regimen. His symptoms resolved, and he regained 18 lbs. He states that he performs self-blood glucose monitoring once or twice a day. The fasting blood glucose values are in the 110 to 125 mg/dL range. Values before supper are 115 to 140 mg/dL (6.3 to 7.8 mmol/L). With treatment, the A1C level improved to the 8.9 to 9.5 range; the most recent value, nine weeks ago, was 9.1 percent.
The patient developed distal sensory neuropathy six months after the diagnosis of diabetes. His symptoms are alleviated by gabapentin but are still present. He has erectile dysfunction. He also has hypertension and gastroesophageal reflux disease. • The patient's examination reveals a blood pressure of 120/70. The heart rate is 60 regular. The body mass index (BMI) 30.6 kg/m2. Peripheral pulses are intact in both lower extremities. Light touch is nearly absent to the knees. Vibration sense is mildly reduced at the great toes, slightly reduced at the medial malleoli, and intact at the tibial tubercles. In addition to metformin, the patient's medications are lisinopril 20 mg once a day,hydrochlorothiazide 25 mg once a day, gabapentin 900 mg three times a day, and aspirin 81 mg once a day
Based on the A1C values, his clinician suspects that the glucose values at home are erroneous. The clinician is concerned that the patient already has distal sensory neuropathy and erectile dysfunction and may develop other complications. The clinician has advised the patient to add glipizide 5 mg before breakfast and supper to his regimen. The patient insists that the glucose readings at home are correct. He has already changed his meter to a different brand and reviewed his testing technique with a diabetes nurse educator. • What is your assessment and plan?
Glucose Monitoring • Plasma Glucose • SMBG(Capillary blood glucose) • CGM • HbA1c • Future technology
Evolution of Diabetes Technology • Glucose Sensors Glucose Meters • REAL- Time monitoring • Incretin-based Therapies • Inhaled Insulin Urine Test Strips Urine Tasting 1900s 1776 1977 1999
Plasma Blood Glucose • FBS • 8 hour fasting(except water) • Postprandial glucose • After first bit
When venous blood is drawn and permitted to clot, the average rate of decrease in serum glucose is approximately 7% or 5-10mg/dlin each hourbecause of glycolysis • It is preferred to prevent reduction in blood glucose as a result of glycolysis by collecting blood into sodium fluoride containing tubes. • Glucose is constant for up to 48 hours in serum or plasma samples when the samples are kept in the refrigerator, after that the amount of glucose will be reduce progressively even at -20oC
Home blood glucose meters measure the glucose in whole blood, while most lab tests measure the glucose in plasma. • Most of the modern meters on the market give results as "plasma equivalent," even though they are measuring whole blood glucose. • Sample sizes vary from 3 to 0.3 μl. • Test times almost 5 seconds.
BLOOD OR PLASMA GLUCOSE • Values for glucose in whole blood are less than in plasma since red blood cells contain only about 8o% water, compared with 93% in plasma, this despite the identical oncentration of glucose in the water phase of both cells and plasma. • Therefore, glucose concentration in plasma is about 12% higher than in whole blood (depending on the haematocrit) • 2 cc • 200 1cc
Common Errors in SMBG • Using expired test strips • Wrong test strips code • Exposing test strips to humidity (leaving bottle open) • Exposing test strips or glucometer to high temperature (eg. Leaving in a car) • Re-using lancets • Inaccurate meter – test annually compared to lab value
Common Errors in SMBG • Too small sample size • American vs. Canadian units • Low battery • Waiting too long before adding blood • Not washing hands before taking sample • Using rubbing alcohol to wash hands
Limitations to SMBG • Complete dependence of parents on their children to do it in our population • In many countries, the cost of SMBG monitoring is very expensive • Discomfort with the measurement
Glucometers: Alternate Site Testing Certain meters allow for testing from “alternative sites” (upper arm, forearm, base of thumb, thigh) • Limitation: blood in tip of finger shows changes in glucose levels faster than blood in other parts of body ** Inappropriate for glucose concentrations after a meal, insulin or exercise, when these values may be changing rapidly
Insulin-treated patients should monitor their blood glucose level at least four times a day Most commonly fasting, before meals, and before bed In addition, patients using insulin can benefit by obtaining postprandial blood glucose readings to help them more accurately adjust their insulin regimen SMBG Use and Frequency
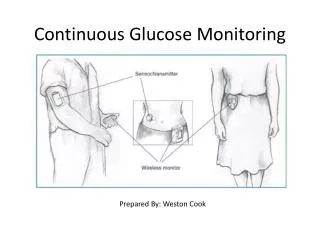
Needle-type Subcutaneous Glucose SensorMinimally invasive sensors use a catheter or a small plastic chip containing a sensor inserted into the subcutaneous space to measure the interstitial glucose. They are replaced every 3-7 days and require calibration 2-3 times daily with SMBG.
Interstitial Fluid Measurement Interstitial fluid glucose (G2) is almost always comparable with blood glucose (G1)
Benefits of CGMS • Immediate feedback - look and learn • BG trend provides more information than static readings • Control + safety
Limitations of CGMS • Interference with glucose readings by sensor can occur with certain substances - i.e.gluthatione, ascorbic acid, uric acid, salicylates • Lag-time for up to 15 minutes when glucose changes rapidly • Overall percentage of error – near 15%
No more glucowatch • Results are affected by sweating and hair • with almost 20 minutes lag as well sensors have to be changed every 20 minutes, with high cost
Haemoglobin Structure of Hb
Haemoglobin • HaemoglobinHbA 97% • HbA2 2.5 % • HbF 0.5% • Several minor haemoglobins migrate more rapidly than HbA in an electric field, called HbA1, made up of : HbA1a + HbA1b + HbA1c
HbA1a1 is fructose-1, 6 diphosphate • HbA1a2 is glucose-6-phosphate attached to the amino terminal of the beta chain. • HbA1b is pyruvic acid linked to the amino terminal valine of the beta chain • HbA1c is condensation of glucose and the N-terminal valine of each beta chain of haemoglobin • Normally less than 6% of Hb is HbA1c
Correlation of MPG & HbA1C Mean Plasma Glucose = (28.7 x HbA1C%) – 46.7
whole blood with EDTA anticoagulant is used • the sample can be stored in the refrigerator for one to three days. • Fasting blood samples is not necessary, however, to avoid interference with fatty acids and lipoproteins in plasma is better to test fast but can be done at any time of the day.
Advantages of HbA1C • Index of long-term control over 120 days and not a snap shot like PG • Can be done at any time of day • Not influenced by diet, exercise, emotional disturbances on test day • Useful index in clinical trials • Useful if missed drugs / default diet • Useful in DD of stress hyperglycemia
Limitations of HbA1C • Cannot be an emergency room test to titrate Insulin or OHA dosage • Cannot register hypoglycemia • if it is elevated it confirms poor control, if it is boarder line, it cannot assure good control in the recent past. • Not sensitive enough for use in GDM • Interfere with many variable
Erythropoiesis • iron deficiency • vitaminB12 deficiency • decreased erythropoiesis Increased HbA1C • iron and VitaminB 12 • therapy with erythropoietin • reticulocytosis, chronic liver disease Decreased HbA1C
Erythrocyte destruction • Increased HbA1C Increased red cell life span (splenectomy) • Decreased HbA1C • Shortened red cell life span(splenomegaly) • certain hemoglobinopathies • rheumatoid arthritis • drugs like antiretrovirals, ribavirin, and dapsone
Glycation • Increased HbA1C • alcoholism • chronic kidney disease • decreased intraerythrocyte pH • Decreased HbA1C • Aspirin (small doses) • certain Hemoglobinopathies Vitamin C, Vitamin E • increased intra-erythrocyte pH
Age AgeHbA1C • Race BLACK > WHITE
Assays • Increased HbA1C • Increased bilirubin • Carbamylated hemoglobin • aspirin (large doses) • alcoholism • chronic opiate use • Decreased HbA1C • hypertriglyceridaemia • Variable HbA1C: Hemoglobinopathies
Various HbA1C assays • Enzymatic method • Immunoassay technique • Ion exchange chromatography(HPLC)gold standard
When to Suspect That a Patient with Diabetes Has a Hemoglobinopathy? • an A1C result is different than expected • an A1C result is above 15 percent • results of self-monitoring of blood glucose have a low correlation with A1C results • a patient’s A1C result is radically different from a previous A1C result following a change in laboratory A1C methods
Case answer The glycated hemoglobin (A1C) level that you ordered returns at 7.1 percent. The report indicates that an abnormal hemoglobin has been detected and suggests the performance of a hemoglobin electrophoresis. This study reveals the presence of 36.6 percent hemoglobin S, consistent with uncomplicated sickle cell trait. You inform the patient, who states that there is no family history of sickle cell trait or disease. You advise him to discuss this with his relatives. His three children, all adults, elect to be screened. One is found to have sickle cell trait. On future laboratory requisitions for A1C assays, you request that the assay be done by boronate affinity chromatography and note the presence of sickle cell trait.
The presence of increased amounts of HbF causes an underestmation of HbA1c by immunoassay. • HPLC is the most accurate method to measure HbA1c levels in patients with high HbF.
Emerging Research About Nanomedicine and Diabetes • nanos(Greek) – one-billionth part of something • nanotechnology - engineering and manufacturing at the scale of a nanometer (10 -9 )
21 December 2009 University of Western Ontario Tears of Joy for Diabetics The non-invasive technology uses extremely small nanoparticles embedded into the hydrogel lenses. These engineered nanoparticles react with glucose molecules found in tears, causing a chemical reaction that changes the color of the lenses.