Download
1 / 14
150 likes | 177 Views
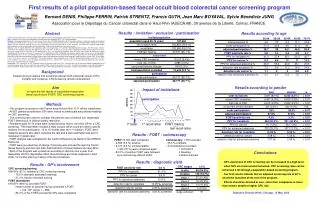
This study examines the effectiveness of immunochemical fecal occult blood tests (FOBTs) in increasing colorectal cancer screening participation. Compared to guaiac-based tests, immunochemical FOBTs do not require dietary restrictions, potentially improving screening rates. Results from studies in Japan suggest higher sensitivity and positive rates with immunochemical FOBTs, making them a viable option for the U.S. population. The low participation in colorectal cancer screenings underscores the importance of adopting immunochemical FOBTs as a more user-friendly alternative.

E N D
Do we need immunochemical fecal occult blood tests in the United States? Tsukasa Namekata, Ph.D., Dr.H.Sc. Director, Pacific Rim Disease Prevention Center and Clinical Associate Professor, University of Washington, Seattle, Washington, U.S.A. Yoshiyuki Watanabe, M.D., Ph.D. Professor, Public Health Research Program, Kyoto Prefectural University of Medicine, Kyoto, Japan Presented at the 2003 Joint Health Conference (of Washington State Public Health Association and Department of Health) held in Yakima, Washington, on October 13-15, 2003
Abstract Colorectal cancer is the second leading cause of cancer-related deaths in the United States. An estimated 147,500 Americans will be diagnosed with colorectal cancer in 2003 and 57,000 will not be survived. Many colorectal cancer deaths can be prevented by screening with a simple and inexpensive fecal occult blood test (FOBT). However, according to the CDC data only 41 percent of Americans 50 years and over underwent colorectal cancer screening within the recommended time intervals. One reason for such a low participation rate can be attributed to the sole use of the guaiac-based FOBT which requires strict dietary restriction. An alternative method is the immunochemical FOBT not requiring dietary restriction. Thus, the purpose of this study is to review published data on performance of the immunochemical FOBT to provide its effective use in screening in the United States. Upon evaluation of studies conducted in Japan where immunochemical FOBTs have been solely used since 1990, it is feasible to use immunological FOBTs in the United States. Considering that no diet restriction is required, immunochemical FOBTs are highly recommended for the U.S. population to increase their participation rate and thereby prevent premature deaths caused by colorectal cancer.
Background • Colorectal cancer is a major public health problem in the United States: the 4th most common type of cancer incidence (129,400 cases) and the 2nd most common cause of cancer deaths (56,600 deaths) in 1999.1 • The 5-year relative survival rate of colorectal cancer, 62%, needs to be improved, and it is much lower than those of prostate (93%) and breast (85%) cancers.1 • Primary prevention has not been effective: a more than 10% increase in overweight adults was observed for the past decade and at present 61% of adults are overweight with 27% obese. This means that more Americans consume high fat and less fiber-contained food and do not exercise enough and all of these are risk factors of colorectal cancer.2
Background, cont. • Colorectal cancer screening rate by fecal occult blood tests (FOBT) among adults 50 years and over remain very low, only about 20% in 2001, as compared with about 80% of women 18 years and older who had a Pap test for cervical cancer screening.3 (See Figure 1) • In the United States the guaiac FOBTs have been mainly used and have required strict diet restrictions which can lead to a low screening participation rate.4,5
Figure 1. Trends in Recent* Fecal Occult Blood Test Prevalence (%), by Gender and Educational Attainment, Adults Aged 50 Years and Older, US, 1997-2001 *a fecal occult blood test within the past year Source: Behavioral Risk Factor Surveillance System, 1996-1997, 1999, 2001, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention and Prevention, 1999, 2000, 2002.
Objective Immunochemical FOBTs, which do not require diet restrictions, are needed to increase screening participants in the United States. Our objective was to review epidemiological studies of immunochemical FOBTs for colorectal cancer screening which were mainly conducted in Japan, where immunochemical FOBTs have been used since 1987 and numerous studies were published to examine effectiveness of such tests.
Results • Immunochemical (IC) FOBTs are superior to Guaiac FOBTs because the IC-FOBTs are designed to detect antibodies specific for human hemoglobin in the lower GI system (or colon and rectum), whereas Guaiac FOBTs react positively to any peroxidase in the feces leading to a high false-positive rate. (Table 1) • High sensitivity to detect colorectal cancer was found in the use of IC-FOBTs than in the use of Guaiac FOBTs in Japan (Table 2). • High positive rates in four methods of IC-FOBTs among colorectal cancer patients were reported in Japan (Table 3). • Sensitivity and specificity to detect colorectal cancer by the 2-day samples of IC-FOBTs were as high as those by the 3-day samples of IC-FOBTs and thus the 2-day-sample approach has been practiced in Japan. (Table 4). • Population screening by the use of IC-FOBTs in Japan showed that detection rates of colorectal cancer were 0.13 - 6.4% and cancers found at an early stage were 43.8 - 74.4% (Table 5).
Table 1. Comparison Between Guaiac FOBTs and Immunochemical FOBTs Adopted from Table 2 of “K Itoh. Fecal occult blood tests. Geka (Surgery) 1990; 52 (12), 1266-1272”6 and modified by Namekata and Watanabe.
Table 2. Comparison of Results Between Guaiac FOBTs and Immunochemical FOBTS Among 2,461 Screening Participants in Tokai University Hospital Source: K Fukushima, et al. Guaiac and immunochemical FOBTs in automatic comprehensive screening. Therapeutic Research 1989;10: 64.7
Table 3. Results of Colorectal Cancer Screening by Four Different Immunnochemical FOBTs (3-day samples) in Japan Note: Each cell indicates FOBT positive cases / screening participants and its rate in %. Adopted from Table 3, Masahiro Tada: Basic and clinical study of immunological fecal occult tests. Therapeutic Research 1989; 10 (suppl. 1): 96-1038
Table 4. Sensitivity and Specificity in Colorectal Cancer Screening by the Use of Immunochemical FOBTs
Table 5. Summary of Study Results Using Immunochemical FOBTs* in Japan *OC-Hemodia was used in all studies except 6. Mtsuda et al who used OC-Sensor and both methods are produced by Eiken Chemical Co. in Tokyo, Japan.
Concluding Remarks • Introducing immunochemical FOBTs is critically important to increase a screening participation rate and can prevent more premature deaths caused by colorectal cancer in the United States. • The recent 5-year relative survival rate of colorectal cancer was 61% among all patient diagnosed both in the U.S. and in Japan but jumped to 91% among patients who participated in screening and found colorectal cancer in Japan.1,20 Thus, it is possible to save most of colorectal cancer patients if detected at an early stage by screening.
References 1.American Cancer Society: Cancer Prevention and Early Detection: Facts and Figures 2003, American Cancer Society 2003. 2. Centers for Disease Control and Prevention: Health, United States, 2002: with Chartbook on Trends in the United States of Americans. DHHS Pub No. 2002-1232 02-0016 (8/02), Dept. of Health & Human Services, 2002. 3. National Center for Chronic Disease Prevention and Health Promotion. Behavioral Risk Factor Surveillance System, 1996-1997, 1999, 2001. Centers for Disease Control and Prevention and Prevention, 1999, 2000, 2002. 4. Cole SR, Young GP: Participation in fecal occult blood test-based screening for colorectal cancer is reduced by dietary restriction. Med J Aust 2001; 175: 195-198. 5. Robinson MHE, Pye G, Thomas WM, et al.: Haemoccult screening for colorectal cancer: The effect of dietary restriction on compliance. Eur J Surg Oncol 1994; 20: 545-548. 6. Itoh K: Fecal occult blood tests. Geka (Surgery) 1990; 52 (12), 1266-1272. (in Japanese) 7. Fukushima K, Kitano S, Yanagi Y, et al. Guaiac and immunochemical FOBTs in automatic comprehensive screening. Therapeutic Research 1989;10: 64-67. (in Japanese) 8. Masahiro Tada: Basic and clinical study of immunological fecal occult tests. Therapitic Research 1989; 10 (suppl. 1): 96-103. (in Japanese) 9. Hirobe K, Owaki T, Matsuzawa Y: 7 years of annual mass screening for colorectal cancer in office workers: usefulness of 3-day RPHA method. Sangyo Eiseigaku Zasshi (J Occ Environ Health) 1995; 37: 187-194. (in Japanese) 10. Mihara S, Kuroda K, Yoshioka R, et al.: Effectiveness and accuracy of colonoscopy and immunochemical FOBTs in colorectal cancer screening. Abstract presented at the 35th Annual Meeting of Japan Gastroenterological Screening Society, Tokyo, Japan in 1996 (Proceeding p.8) (in Japanese) 11. Sado M, Mihara S, Kawazu S, et al.: Accuracy of colorectal cancer screening and analysis of false negative cases. Abstract presented at the 35th Annual Meeting of Japan Gastroenterological Screening Society, Tokyo, Japan in 1996 (Proceeding p.20) (in Japanese) 12. Miyazaki S, Mihara S, Kuroda K, et al.: Analysis of false negative cases of colorectal cancer in mass screening. Abstract presented at the 35th Annual Meeting of Japan Gastroenterological Screening Society, Tokyo, Japan in 1996 (Proceeding p.17) (in Japanese) 13. Tanimoto T, Yoshihara M, Sumii K, et al.: An evaluation on mass screening for colorectal cancer with further examination. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1996; 34:1-6. (in Japanese) 14. Tanimoto T, Yoshihara M, Sumii K, et al.: The system of colorectal mass survey and the rate of further examination. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1997; 35: 7-11. (in Japanese) 15. Orii F, Satoh T, Taniguchi M, et al.: An evaluation of gastroenterological mass survey in Memuro Town. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1996; 34: 17-22. (in Japanese) 16. Inamoto Y, Kawamura S, Arimoto S, et al.: The accuracy of work-up examinations in colorectal cancer mass screening in Yamaguchi Prefecture. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1996; 34: 23-28. (in Japanese) 17. Yoshii Y: Present status and problems in mass screening for colorectal cancer in Nagoya City. Therapeutic Research 1996: 17: (suppl. 2) S309-312. (in Japanese) 18. Matsuda K, Takeda T, Yamazaki S: Accuracy of the further examination in the mass screening for colorectal cancer: Follow-up study by means of a record linkage with the Fukui Cancer Registry. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1996; 34: 342-347. (in Japanese) 19. Suda T, Nakano M, Iniue S, et al. Present status of mass screening programs of colorectal cancer in Omiya City and investigation of quantitative system of fecal hemoglobin density significant for colorectal cancer detection. Nihon Shokaki Shudan Kenshin Shi (Japan JMass screening of Gastro-intestinal Tracts) 1997; 35: 671-680. (in Japanese) 20. Hisamitsu S, Ishiguro T, Tsuji I, et al.: Evaluation of Validity of New Cancer Screening Methods. Japan Public Health Association 2000. Table 3 in p. 32 and Table 9 in p.35.