Download
1 / 28
280 likes | 298 Views
Explore the HIV epidemic overview and prevention strategies in South Africa, focusing on key populations like sex workers and the government's policies to combat HIV/AIDS. Learn about prevention targets, key population statistics, and essential policies in place.

E N D
HIV Prevention and Policies in South Africa Dr. Yogan Pillay Global Prevention Coalition Meeting 10-11 October 2017
Epidemic overview • In 2016, there were an estimated 7 100 000 [6 400 000 – 7 800 000] people living with HIV in South Africa. • New HIV infections declined by 29% between 2010 and 2016, with an estimated 270 000 [240 000 – 290 000] new HIV infections in 2016. • An estimated 110 000 [88 000 – 140 000] people died of AIDS-related causes in 2016, a 49% decline from 2010. • Adult women (15+ years) comprise 61% of the people living with HIV in South Africa, and 58% of new infections and 50% of deaths. • There were equal number of deaths among adult men and women aged 15+ years. • New HIV infections among children (0-14 years) have more than halved between 2010 and 2016, with an estimated 12 000 [9 600 – 22 000] new HIV infections in 2016.
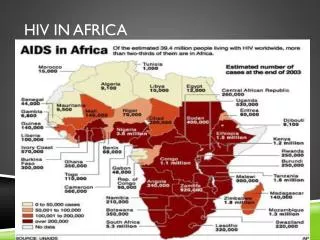
34% of new HIV infections in ESA occur in South Africa, while another nearly 50% occur in 7 countries - Mozambique, Kenya, Zambia, United Republic of Tanzania, Uganda, Zimbabwe and Malawi Kenya 8% Zambia 8% Rest of region (11 countries) 17% South Africa 34% Uganda 7% Zimbabwe Tanzania 5% 7% Mozambique 11% Malawi 5% Source: UNAIDS Estimates 2017
Some populations are being left behind The most recent data indicates that two populations in particular have the highest proportion of new infections and are being left behind: Adolescent girls and young women Key populations: men who have sex with men (MSM) and female sex workers
Key populations • HIV prevalence among sex workers was estimated to be 57.7%, as compared to a national HIV prevalence of 23.8% among 15-49 females. However, there are large differences by location and age. • The SAHMS Study, 2014 estimated HIV prevalence among female sex workers at 71.8% in Johannesburg; 39.7% in Cape Town, and 53.5% in eThekweni with differences in among female sex workers 25+ years compared to 16-24 age group, confirming the urgency of focused intervention for sex workers from an early age.
There are 153 000 sex workers in South Africa at substantial risk of HIV Figure 1: Provincial distribution of sex workers in South Africa • The 153 000 sex workers are comprised as follows: • 138 000 female • 7 000 male • 6 000 transgender Sex workers often work in hotspots around mines, military zones, harbours and along transport routes Figure 2: Distribution across rural and urban areas
There are 8 goals in the NSP, Goals 1, 3, 4, and 5 are linked to prevention
Several Strategies and Plans linked to the NSP 2017-22 address HIV prevention have been developed and implemented • National Health Sector HIV Prevention Strategy • National Sex Worker HIV Plan • National LGBTI Plan • Department of Basic Education HIV Policy • Learner Pregnancy Policy • Integrated School HP policy • Adolescent & Youth Health Policy • Department of Social Development HIV prevention policy
The Health Sector HIV Prevention Strategy with the aim of guiding and accelerating implementation of Combination HIV prevention interventions in support of the national strategic plan (NSP) for HIV and AIDS and TB 2017-2022. • The strategy will assist district managers and implementers plan and implement targeted combination prevention interventions (biomedical and non-biomedical) specific to different target groups • Combination HIV prevention: No single intervention can bring an HIV epidemic under control on its own, but an optimal set of interventions, implemented well and on a large scale, can significantly reduce HIV incidence. • NSP prevention targets: 270000-100000 annually: Young women and girls: 2000-800 weekly
Background on young people • Youth 36% of the S African population • Young persons ages 15-34 made up ~70% of total unemployment over the last decade • Not in Employment, Education or Training (NEET) rate for youth 30% in 2012, highest rate recorded at 33,5% in 2013 • The proportion of economically active youth declined over the last five years (2009 – 2014) • Youth without a matric are most likely to be unemployed and hence the need for focus on keeping girls in school until matric • Young people living in rural areas continue to bear the brunt of unemployment.
Age of consent for access to sexual and reproductive health services Age of consent to sexual activity Age of marriage Social protection Best practice: “She Conquers Campaign” Policies to create an enabling environment for adolescent girls and young women include
Enabling environments for Adolescent Girls and Young Women • The South African Children’s Act of 2005 provides that a child aged 12 years or older may consent to medical treatment without parental consent if he/she is of sufficient maturity and stage of development. Parental consent to abortion is not required, irrespective of the age of the child. • In South Africa, consensual sexual acts among adolescents are decriminalized as long as the age difference is not more than two years. • In South Africa, the Children’s Act 28 of 2005 set the minimum age of marriage at 18 years. • South Africa has integrated comprehensive sexuality education (CSE) for in- and out-of-school youth. • Policy Framework for Social Security for Youth in South Africa that will link them to education and employment • However, adolescent girls and young women 15-24 continue to account for 33% of new infections among adults 15-49 and according to the latest DHS 2016, teenage pregnancy is 16% and has remained unchanged since 1998.
The enabling environment for Adolescent Girls and Young Women in South Africa currently: • The Adolescent & Youth Health Policy 2016-2020 (AYHP) identifies six principal objectives than integrate mental health and wellbeing of AY, provides comprehensive, integrated SRH Services, test and treat for HIV/AIDS and TB, reduce substance abuse and violence, promote healthy nutrition and reduce obesity, and empowers adolescents and youth to engage with policy and programming on youth health. • The Integrated School Health Policy (ISHP): this policy includes anintegrated HIV & SRH component consisting of comprehensive sexuality education, condoms, contraceptives and HIV counselling and testing at schools. Rollout will start with selected secondary schools in high priority areas. • She Conquers Campaign (adolescent girls and young women) These recent policies integrate the enabling environment policies outline previously.
Emerging issues to consider • How many adolescent girls and young women are at risk of HIV and pregnancy in 22 sub-districts? How many have been reached in the first year – how will the remainder be reached? • How many secondary schools have been reached with IEC, condoms, HTS etc. and how many more need to be reached? How many clinics are youth friendly and how many more need to be reached? • Need to accelerate provision of comprehensive package of services in the 22 sub-districts already prioritized. Scale-up DREAMS. • Need to find ways of identifying individual adolescent girls and young women at risk for HIV infection and link them to services to enhance their resilience.
Key populations: Female sex workers and men who have sex with men
On the 11th March 2016, the Deputy president launched a national plan to respond comprehensively to sex workers
Sex workers Decriminalisation of sex work Abolish restrictions that exclude people with criminal records from securing social services Repeal of laws that place people who engage in the sex trade in state sex offender registries Stop using condoms as evidence and cause for arrest. Curb laws used to criminalize people who engage in the sex trade Access to sexual and reproductive health services Social protection Men who have sex with other men Abolition of sodomy as a crime Legalize same sex marriage Access to psychosocial and health services Social protection Steps to created an enabling environment for key populations in South Africa include:
Sex work is still criminalized in South Africa. The South African National Sex Worker Plan 2016-2019 (linked to the Health Sector Prevention Strategy) outlines steps to secure political commitment for the decriminalisation of sex work to achieve public health goals and to safeguard human rights, work with SAPS to eliminate the practice of using possession of condoms, lubricant, ART, or other legal commodities as evidence of sex work and grounds for confiscation or arrest. The National Sex Work Plan also provide steps towards building a social capital package, Community empowerment, Economic empowerment (including capacity building), and a 3-tiered delivery approach, supported by peer educators, based on the density of sex workers to provide them access to sexual and reproductive health services with HIV prevention, screening and treatment delivered in hotspots by sex worker peer educators and access to flexible services. The enabling environment for Sex workers in South Africa currently:
Men who have sex with other men Sodomy was abolished in 1998 and same sex marriage has been legalized However, lack of access to necessary prevention commodities such as condom-compatible lubricants, lack of knowledge on the part of health care and social services professionals about LGBTI specific health, exclusion from equal opportunity to participate in the economy, and internalised stigma all contribute to LGBTI people’s vulnerability to HIV, TB and STIs. South African National LGBTI HIV Plan, 2017-2022 (LGBTI HIV Plan) is a milestone in the country’s response to HIV, AIDS, STIs, and TB. It is in line with the NSP 2017-2022 and Health Sector Prevention Strategy 2016. The enabling environment for MSM in South Africa currently:
The National Plan provides a package of LGBTI-appropriate HIV, STIs and TB-related health care services to 200 000 LGBTI people; Health: Initiating 5,000 MSM and trans people on PrEP; use condoms and condom-compatible lubrication correctly and consistently; and ensuring that all LGBTI have access to comprehensive services (self-testing) Empowerment of MSM populations through a peer-led programmes Psychosocial support - reduce internalised and external stigma and discrimination Human rights - develop and implement effective mechanisms to deal with human rights abuses and violence The enabling environment for MSM in South Africa currently, continued:
How many MSM are we reaching currently and how many not? A need for key population estimates. Where are they and how to reach them, in townships, informal settlements? How do we expand testing in this population? What percent of MSM have tested and those tested positive how many are on ART? Given the results of the PrEP demonstration projects in MSM sites should we consider expansion and to which sites? How to promote regular testing and consistent condom use in MSM populations? Consider diagnosis of acute HIV infection and immediate initiation on treatment (with consistent condom) use should decrease onward transmission. Emerging issues to consider for key populations in South Africa
Questions that remain unanswered by current policies • How many people are still at risk for HIV infection and are not receiving prevention information and services. • There is no easily defined cascade for prevention • Not all South Africans are equally vulnerable to HIV infection • The majority of South Africans are negative – how do we keep them negative; how do we get those with HIV tested and on treatment as soon as possible? • Do we know who are at risk for HIV infection but do not currently have access to prevention services? How can we better target our prevention services? How many sex workers and MSM are not being reached?
Lessons learnt • While policy and legal environment are critical, on their own they are not sufficient to turn the tide in reducing new infections and reaching epidemic control. • Challenges around implementing these policies throughout the country possibly contribute to a slowed pace in meeting prevention targets. • Alignment of policies across sectors such as education and health can contribute to both improved outcomes in education attainment and health for young people. • It is important to complement policy with comprehensive programming and appropriate coordination and involvement of the concerned populations.
Concluding remarks: • South Africa has done well in creating an enabling environment but it will be important that all sectors work together for the realisation of combination prevention, demand generation and addressing inequalities • Strengthening programming at all levels is critical to reap the benefits of good policies. • Prevention cascades for the various interventions should be considered by exploring lessons learnt from PMTCT and 90-90-90 for a similar type of approach intervention by intervention so that prevention work is more systematic and more targeted for impact.