1 / 70
700 likes | 771 Views
Adrenal Insufficiency: Evaluation and Management

E N D
Adrenal Insufficiency Dr Shahjada Selim Associate Professor, Department of Endocrinology, BSMMUVisiting Professor in Endocrinology, Texila American University, USAEmail: selimshahjada@gmail.com, info@shahjadaselim.com
Introduction Adrenal insufficiency (AI) comprises a fairly large group of disorders characterized by (inappropriately) low production of glucocorticoids (GC) with or without low production of mineralocorticoids (MC). Destruction or the dysfunction of the adrenal cortex mainly causes glucocorticoid and mineralocorticoid deficiency. Primary AI is also known as autoimmune adrenalitis or Addison disease.
Introduction AI ranges from mild nonspecific symptoms to life-threatening shock conditions. Due to its vague symptoms and varying degree of clinical presentation, a clinician must maintain a high level of suspicion for this disease [1]. The decreasing or suppressed adrenal function may be masked until stress or illness triggers an adrenal crisis [2]. • Ceccato F,Scaroni C, Central adrenal insufficiency: open issues regarding diagnosis and glucocorticoid treatment. Clinical chemistry and laboratory medicine. 2018 Nov 14] • Shaffer ML,Baud O,Lacaze-Masmonteil T,Peltoniemi OM,Bonsante F,Watterberg KL, Effect of Prophylaxis for Early Adrenal Insufficiency Using Low-Dose Hydrocortisone in Very Preterm Infants: An Individual Patient Data Meta-Analysis. The Journal of pediatrics. 2018 Nov 8
Classification AI can be classified into • Primary, • Secondary, and • Tertiary causes.
Primary Adrenal Insufficiency Primary AI occurs when there is a pathology affecting the adrenal gland itself. It affects glucocorticoid and mineralocorticoid function. The onset of disease usually occurs when 90% or more of both adrenal cortices are dysfunctional or destroyed.
In 1855, Dr Thomas Addison (April 1793 – 29 June 1860) described: “…a morbid state, the leading and characteristicfeatures of which are anemia, general languor and debility,remarkable feebleness of the heart’s action, irritabilityof the stomach and a peculiar change of color of the skin, occurringin connection with a diseased condition of the suprarenal capsules”
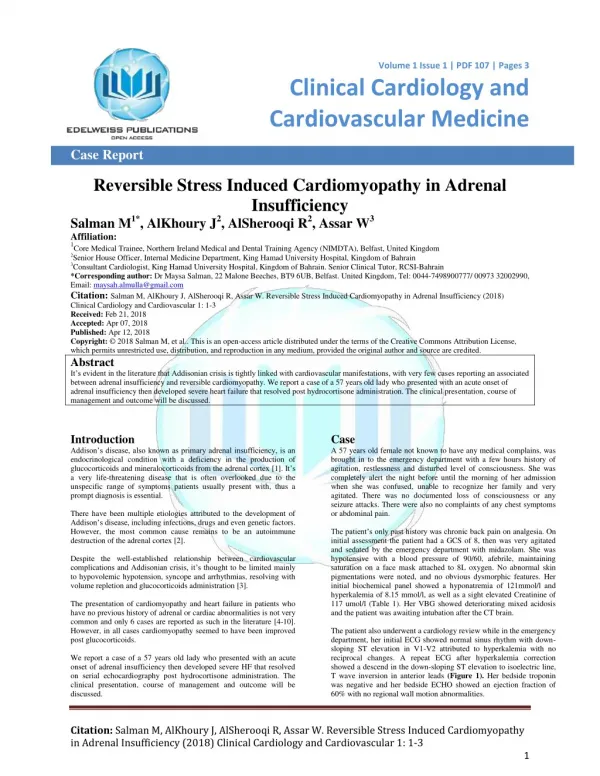
In contrast, an acute adrenal crisis can manifest with vomiting, abdominal pain, and hypovolemic shock. Loriaux et al. Curr Opin Endocrinol Diabetes Obes. 2009; 16(5):392-400 (ISSN: 1752-2978)Loriaux DL; Fleseriu M
Epidemiology As many as 144 million individuals in the developed world may have Addison disease. When treated properly, patients can have a roughly normal lifespan. Untreated patients have a high mortality rate. The autoimmune form of adrenal insufficiency has a male-female predisposition based on the type of autoimmune condition. Females are more likely to have the polyglandular form while isolated adrenal damage is more common in males in the first two decades. By the fourth decade, the isolated form is more common in women. 1.Rushworth RL et al. Hormone research in paediatrics. 2018
….Epidemiology Due to the diverse causes of AI, no distinct group of individuals is at increased risk of disease. The epidemiology of AI in children is not well-defined. Congenital adrenal hyperplasia (CAH) is the most common etiology of primary adrenal insufficiency in children, occurring once in 14,200 live births [1]. 1. Meyer et al. Deutsche medizinische Wochenschrift (1946). 2018 Mar
Pathophysiology The pathophysiology of AI depends on the etiology. With most forms of autoimmune (primary) adrenal insufficiency, the patient has antibodies that attack various enzymes in the adrenal cortex (though cell-mediated mechanisms also contribute). Various genetic factors have been identified that play a role in the development of primary adrenal insufficiency or autoimmune adrenalitis. These include the major histocompatibility complex (MHC) haplotypes DR3-DQ2 and DR4-DQ8 [1]. 1. Mitchell et al. Nature reviews. Endocrinology. 2012 Jan 31
…Pathophysiology Secondary AI refers to decreased adrenocorticotropic hormone (ACTH) stimulation of the adrenal cortex and therefore does not affect aldosterone levels. Traumatic brain injury (TBI) and panhypopituitarism are common causes [1]. • Alexandraki KI,Grossman A, Management of Hypopituitarism. Journal of clinical medicine. 2019 Dec 5
…Pathophysiology Tertiary AI refers to decreased hypothalamic stimulation of the pituitary to secrete ACTH. Exogenous steroid administration is the most common cause of tertiary adrenal insufficiency. Surgery to correct Cushing disease can also lead to tertiary adrenal insufficiency [1]. • Alexandraki KI,Grossman A, Management of Hypopituitarism. Journal of clinical medicine. 2019 Dec 5
Histopathology Histopathology varies according to the pathological process involved in adrenal gland dysfunction. In autoimmune adrenalitis, there is atrophy of the adrenal gland with infiltration of lymphocytes along with fibrosis of the adrenal capsule. As AI is caused by dysfunction of the cortex, the adrenal medulla is not affected and is spared [1]. 1. Guo et al. European journal of radiology. 2007 Apr
Histopathology AI due to TB results in enlargement of the adrenal glands with the presence of caseating granulomas. The adrenal medulla is usually not spared, and the gland is characterized by diffuse calcification. In patients with AIDS, there is infarction, hemorrhage, and necrotizing inflammation of the adrenal gland [1]. 1. Guo et al. European journal of radiology. 2007 Apr
Auricular-Cartilage Calcification • Calcification of the Auricular Cartilages Occurs in Primary or Secondary Adrenal Insufficiency • Occurs Mostly in Males
Psychiatric Manifestations • Impairment of Memory • Depression • Psychosis
Mineralocorticoid Deficiency: • Salt Craving • Increased Thirst for Ice Cold Liquids • Hyperkalemia With a Mild Hyperchloremic Acidosis • Hyponatremia: Inappropriate ADH Secretion Due To Cortisol Deficiency; Salt Wasting
Cardiovascular • Hypotension • Postural Dizziness or Syncope The Presence of Hypertension Is Strong Evidence Against a Diagnosis of AI!
Sexual Dysfunction • Decreased Axillary and Pubic Hair and Loss of Libido Are Common in Women • Amenorrhea in 25% of Women
Diagnosis • Are the Adrenals Functioning? • If Not, Why Not?
Diagnosis Are the Adrenals Functioning? - Cortisol Concentration - Adrenal Stimulation Testing
Baseline Cortisol Concentration • Highest Cortisol Concentration Between 4:00AM - 8:00 AM • < 3 µg/dl [83nmol/L] Insufficiency • < 10 µg/dl [270nmol/L] Suggests Adrenal Insufficiency • But…. If Corticosteroid-Binding Globulin Deficiency, Interpretation May Be Incorrect
Cosyntropin Stimulation Test (SST) • 250 ug ACTH, IV or IM • Cortisol Measured 30 and 60 Minutes Later • Level > 18-20 µg/dl [500-540nmol/L] Normal • Can Be Done At Any Time During The Day
Secondary Adrenal Insufficiency:Diagnosis • Recent Onset Adrenal Glands May Respond To ACTH Stimulation • Time Needed for the Adrenal Glands to Become Unresponsive Varies
Testing In Adrenal Insufficiency Adrenal Insufficiency Primary Secondary Normal Recent Onset 20 Adrenal Insufficiency ACTH pg/ml @ 8 AM Serum Cortisol mg/dl Long-Standing 20 Adrenal Insufficiency 10 Adrenal Insufficiency 0 30 60 = Normal Range Time minutes
Secondary Adrenal Insufficiency The Best Way To Stimulate Endogenous ACTH… Insulin Tolerance test Metyrapone Stimulation Test CRH Stimulation Test
Insulin Tolerance Test (ITT) The Gold Standard Test • Glucose Level <40 mg/dl [2.2 mmoml/L] After Insulin IV • Cortisol Level > 18-20 µg/dl [500-540 nmol/l] • This Test Should Not Be Done In Patients With Seizures or Severe Cardiac Disease
Cortisol < 7ug/dl [192 nmol/L] and 11Deoxycortisol > 10ug/dl
The Metyrapone Test A normal response is a rise in 11-deoxycortisol concentrations to more than 10.5 mcg/dL 4 hours after the last dose of metyrapone is given or a 2-fold to 3-fold increase in 24-hour urinary concentrations of 17-hydroxycorticosteroid (which include tetrahydro compound S, a urinary metabolite of 11-deoxycortisol) on the day of or the day after the administration of metyrapone. Standard metyrapone stimulation tests involve administering metyrapone 300 mg/m2 in 6 divided doses over 24 hours. Because metyrapone inhibits 11-hydroxylase, which is involved in the last enzymatic step in cortisol synthesis, plasma levels of the cortisol precursor, 11-deoxycortisol, increase. This test is cumbersome and carries some risk of inducing an adrenal crisis.
Imaging Studies Chest radiograph: • The chest radiograph may be normal but often reveals a small heart. • Stigmata of earlier infection or current evidence of TB or fungal infection may be present when this is the cause of Addison disease.
Imaging Studies CT scan: • Abdominal CT scan may be normal but may show bilateral enlargement of the adrenal glands in patients with Addison disease because of TB, fungal infections, adrenal hemorrhage, or infiltrating diseases involving the adrenal glands. • In Addison disease due to TB or histoplasmosis, evidence of calcification involving both adrenal glands may be present. • In idiopathic autoimmune Addison disease, the adrenal glands usually are atrophic.
Other Tests ECG may show low-voltage QRS tracing with nonspecific ST-T wave changes and/or changes due to hyperkalemia. These changes are reversible with glucocorticoid replacement. Sputum examination, examination of gastric washings for acid-fast and alcohol-fast bacilli, and a Mantoux or purified protein derivative (PPD) skin test may be needed if TB is thought to be the cause.
Histologic Findings In cases due to idiopathic autoimmune adrenocortical atrophy, the adrenal glands usually are atrophic, with marked lymphocytic infiltration and fibrosis of the adrenal capsule. The adrenal medulla is spared. In cases due to TB, the adrenal glands may be enlarged and contain caseating granulomas. Diffuse calcification may be evident, and the adrenal medulla usually is involved. [17] In patients with AIDS, the adrenal glands may show necrotizing inflammation, hemorrhage, and infarction.
Adrenal Insufficiency:Evaluation of Patient at Risk (History of Steroid Administration) • Serum Cortisol (6-8 am) • Cortrosyn Stimulation Test (≥ 18 ug/dl) [500 nmol/L] • Insulin Tolerance Test (≥ 18 ug/dl) [500 nmol/L] • Metyrapone Test • CRH Stimulation Test
Diagnosis of Adrenal Insufficiency in Critical Illness “Relative” Insufficiency
Evaluation of Adrenal Insufficiency in Critical Illness • Glucocorticoid secretion increases during critical illness, yet the increase may not be detected if only total cortisol concentrations are measured. • Serum free cortisol measurements may be helpful to avoid unnecessary glucocorticoid therapy. • These assays are not yet widely available.
Evaluation of Adrenal Insufficiency in Critical Illness: A Reasonable Approach Critical Illness: Random Cortisol < 15 ug/ml 15-34 ug/ml > 34 ug/l AI Likely Free Cortisol & Treat Cortrosyn Stim Test AI Unlikely < 9 ug/ml ≥ 9 ug/ml
Evaluation of Adrenal Insufficiency in Critical Illness: The Bottom Line While some critically ill patients may have functional adrenal insufficiency, there is currently no consensus on diagnostic criteria or indications for treatment.
Treatment • Chronic Adrenal Insufficiency • Acute Adrenal Insufficiency
Chronic Treatment • Hydrocortisone: Short Acting • Cortisone Acetate: Short Acting, But Needs Liver Conversion to Become Active • Prednisone: Long Acting • Dexamethasone: Very Long Acting
Steroid Preparations Steroid Half Life Glucocorticoid Mineralocorticoid (minutes) Potency Potency Hydrocortisone 90 1.0 1.0 Cortisone 30 0.8 0.8 Prednisolone 230 4.0 0.8 Prednisone 60 3.5-4.0 0.5 Dexamethasone 280 25.0-30.0 0.0