Download
1 / 45
460 likes | 771 Views
CYSTIC TUMORS OF THE PANCREAS. A.R.Fahim,M.D 5,day,92. Less than 10% of pancreatic neoplasms Results of 24,000 abdominal CT and MRI during 8-year period: pancreatic cysts in 1.2% of patients 60% cystic neoplasms MCNs, serous cystadenomas , and IPMNs comprise more than 80%

E N D
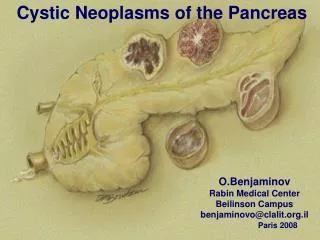
CYSTIC TUMORS OF THE PANCREAS A.R.Fahim,M.D 5,day,92
Less than 10% of pancreatic neoplasms • Results of 24,000 abdominal CT and MRI during 8-year period: pancreatic cysts in 1.2% of patients 60% cystic neoplasms • MCNs, serous cystadenomas, and IPMNs comprise more than 80% • Masquerade as pancreatic pseudocysts • High cure rate following surgical treatment
DIFFERENTIAL DIAGNOSIS Exclusion of a pancreatic pseudocyst: • lack an epithelial lining • history of acute or chronic pancreatitis, or abdominal trauma • lack of septae, loculations, solid components, or cyst wall calcifications on CT or MRI • communication between the cyst and the main pancreatic duct • high levels of amylase
Does require surgical resection? • Slow growing, and favorable prognoses • Tumors with malignant potential include MCNs, IPMNs, solid pseudopapillary tumors (SPTs), and cystic islet cell tumors • Serous cystadenomas are almost universally benign
Many of these cysts are very small (<2 cm) • Nonoperation • Operation: older than 70 years new symptoms cyst growth on serial imaging
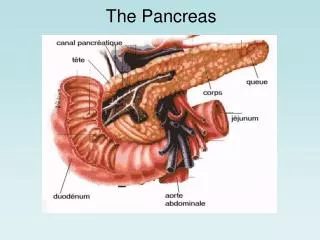
DIAGNOSTIC IMAGING • CT • MRI • ERCP • EUS • PET
MUCINOUS CYSTIC NEOPLASMS • 10% to 45% • Thick-walled with occasional septations • Filled with thick mucous or hemorrhagic material • Benign, borderline, or malignant (cystadenocarcinoma) • All these tumors should be treated as premalignant lesions • Ovarian-type stroma
Almost exclusively in women • Confined to the distal pancreas (body and tail of the gland) • Never multifocal • Mean age is 50 years • Abdominal pain or a palpable mass • Incidental:25%
MCN should be suspected when a CT or MRI of the abdomen shows a cyst within the body or tail of the pancreas in a middle-aged woman • No communication between the pancreatic duct and the cyst itself • EUS can identify septations and cyst wall nodules and allows cyst wall biopsy and cyst fluid aspiration
Classification : benign adenomas (72%) borderline neoplasms (10.5%) carcinoma in situ (5.5%) invasive cancer (12%) • Malignant MCNs larger than benign counterparts (80 vs. 45 mm) more likely to harbor nodules within their walls
Surgical resection is advocated for all of them • Distal pancreatectomy with or without splenectomy • Laparoscopic approach is acceptable • Lymph nodes metastases are rare
Given that MCNs are never multifocal, long-term surveillance is not required for patients with resected noninvasive tumors
SEROUS CYSTADENOMAS • Microcystic adenoma • Second most common • Women (75%) • Mean age of 62 years • Most (50% to 70%) occur in the body or tail • Association with von Hippel-Lindau disease • Vague abdominal pain and discomfort, palpable mass,incidental
Numerous tiny cysts separated by delicate fibrous septa, giving them a honeycomb appearance • The cysts are filled with clear watery fluid and are often arranged around a central stellate scar that may be calcified • Spongy mass with a central “sunburst” calcification in CT:10%
Benign • Surgical resection is the treatment of choice for symptomatic lesions
Observation if asymptomatic. • Observation carries the risk of continued growth, which may lead to complications such as hemorrhage, obstructive jaundice, pancreatic insufficiency, or gastric outlet obstruction • Tumors larger than 4 cm: resction
INTRADUCTAL PAPILLARY MUCINOUS NEOPLASMS • IPMNs represent papillary neoplasms within the main pancreatic duct • Benign (adenoma), borderline, or malignant(60%) • Lymph node metastases( 33% to 51%)
Men=women • Median age 65 years • Abdominal pain and weight loss • Recurrent pancreatitis: 20% • Acute pancreatitis:25% • Malignant neoplasms:older,jaundiceor new-onset diabetes
CT or MRI: dilation of the pancreatic duct • ERCP:patulousampulla of Vater with extruding mucus(fish mouth) main duct dilation filling defects due to viscid mucus or tumor nodules communication between cystic areas and the main pancreatic duct
Pancreaticoduodenectomy • Distal pancreatectomy • Total pancreatectomy
SOLID PSEUDOPAPILLARY TUMORS • Less than 10% of the cystic tumors • Women:men(10 : 1 ratio) • Disease of young women in their 30s • Abdominal pain:50% • Large abdominal mass:35% • Incidental:15% • Body and tail:60%
Carcinoma:20% • Complete loss of E-cadherin expression in the cells or abnormal localization of E-cadherin to the cell nucleus:100% • Very slow-growing • Complete resection