1 / 12
120 likes | 215 Views
Dr Vivek Baliga discusses frozen shoulder, and how it can be managed easily and safely.

E N D
Frozen Shoulder - A Review Dr Vivek Baliga Consultant Physician Baliga Diagnostics
What Is Frozen Shoulder? • Also called adhesive capsulitis • Clinical condition where the movement of the shoulder becomes restricted • Range from mild restriction all the way to severe restriction accompanied by a great deal of pain • First recorded case of frozen shoulder was described in 1872 by Duplay in this article on ‘periarthritis scapulohumeral’. • The term ‘frozen shoulder’ was coined by Codman in 1934.
Incidence Of Frozen Shoulder • 3 to 5% incidence of frozen shoulder in the general population. • Those who have diabetes can have up to a 20% incidence • One of the most common clinical conditions encountered by orthopaedic surgeons. • Typical patient who has frozen shoulder is a woman between the age of 50 to 70 years
Associated Conditions • Diabetes mellitus • Hyperthyroidism • Hypothyroidism • Heart disease (cardiovascular disease) • Tuberculosis • Parkinson’s Disease • Stroke - Immobility • History of injury to the arm - tears, fractures etc.
Classification • Primary Frozen Shoulder • Idiopathic frozen shoulder is insidious in onset • Secondary frozen shoulder • Follows trauma or injury to the shoulder joint and subsequent requirement for immobilisation.
Clinical Stages Frozen or Transitional stage • Pain remains constant • Range of movement of the shoulder joint becomes limited • Lasts between 4 to 12 months Thawing stage • Range of movement returns to normal gradually over a 12 to 42 month period. Freezing or Painful stage • Mild restriction of the shoulder joint • Patients may not necessarily seek medical attention.
Symptoms • Gradual onset shoulder pain • Inability to lift the arm up beyond a certain point - abduction and external rotation becomes painful • Discomfort localised to the area of insertion of deltoid muscle • Inability to sleep on the affected side • Normal shoulder x-ray
Diagnosis A diagnosis of frozen shoulder is often made clinically. X-rays may not necessarily be helpful. Blood tests may determine other associated conditions. There is usually no specific need for an MRI scan as a clinical diagnosis is often sufficient.
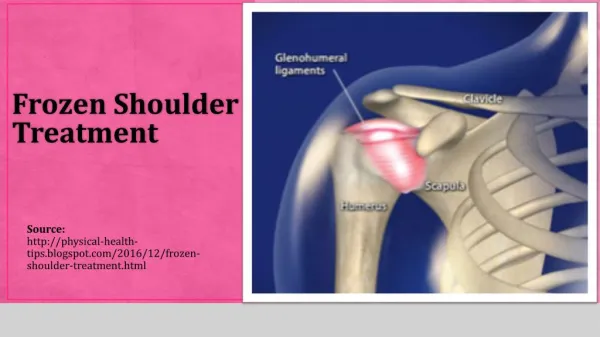
Treatment • Non-Operative • Operative
Non-Operative Treatment • Non-steroidal anti-inflammatory drugs can help relieve pain to an extent and remain the first choice of treatment. • They do not change the natural course of the disease. • Intra-articular corticosteroid injections • There may be some short-term benefit. • Subacromial or glenohumeral approach is considered • Exercise Therapy • Aim behind exercise therapy is to prevent a further reduction in the range of movement of the shoulder joint. • Exercises include passive mobilisation and capsular stretching.
Surgical Treatment • Surgical treatment is only recommended in those individuals who have not seen any difference in their symptoms following at least 2 months of nonsurgical therapies. • Manipulation under anaesthesia • Individual is placed under anaesthesia and the shoulder joint is manipulated so as to loosen the tissues and allow full range of movement. • Arthroscopic release and repair • The tightened coracohumeral ligament and contracted capsule can be loosened and released
Conclusion • Frozen shoulder is a common condition that carries a significant morbidity. • Treatments revolve around non-surgical methods in combination with steroid agents. • However, a small number of patients will require surgical release of the shoulder capsule for complete benefit. References Uppal HS, Evans JP, Smith C. Frozen shoulder: A systematic review of therapeutic options. World Journal of Orthopedics. 2015;6(2):263-268. doi:10.5312/wjo.v6.i2.263.