Download
1 / 35
350 likes | 364 Views
Learn about Acute Suppurative Otitis Media & its stages, pathophysiology, clinical features, and management. Explore risk factors, etiology, complications, diagnostic evaluation, and treatment options.

E N D
UNIT-1OTITIS MEDIA PRESENTED BY: Ms. Pavithra K Lecturer, MSN dept
LEARNING OBJECTIVES At the end of the class students will be able to • define ASOM • enlist the types of otitis media • explain the stages the ASOM • describe the patho-physiology of ASOM • list down the clinical features of ASOM • enumerate the management of ASOM
INTRODUCTION • An infection of the air-filled space behind the eardrum (the middle ear). • Infection or inflammation of the middle ear cleft mucosa • Second most common disease diagnosed in young children • Chronic otitisexterna left untreated
TYPES • Acute Suppurativeotitis media (ASOM) • Acute • Rapid onset of signs and symptoms • Less than 3 week • Sub Acute • 3 weeks to 3 months • Chronic Suppurativeotitis media (CSOM) • 3 months or longer
OTHER TYPES OM with effusion • Otitis media with effusion (OME), also known as serous otitis media (SOM) or secretoryotitis media (SOM), and 'glue ear • Fluid or discharge accumulation that can occur in the middle ear Adhesive otitis media • Adhesive otitis media is when thin retracted ear drum becomes sucked into the middle-ear space and stuck to the ossicles of the middle ear.
Acute otitis media • Infection and inflammation of the middle ear between 3 weeks to 3 months
RISK FACTORS • Age • Non-breastfed children • Pacifier use • Contaminated food • Genetic factors: Increased incidence among twins • Socio- economic conditions • Season-winter. • Underlying disease (cleft palate, allergic rhinitis) • Family history of otitis media • Hygiene • Otitisexterna
ETIOLOGY Bacteria • Streptococcus pneumoniae • Haemophilusinfluenzae • Moraxellacatarrhalis • Group A streptococcus.
Eustachian tube • Adenoiditis • Tonsillitis • Rhinitis • Sinusitis • Pharyngitis • Infection secondary to cleft palate
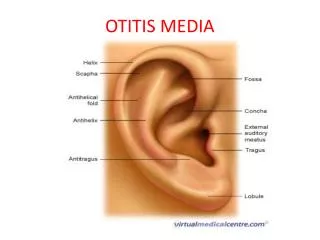
External ear • Otitisexterna • Sharp foriegn body • Trauma to the tympanic membrane • Tympanic membrane perforation Other causes • Head injury • Barotrauma • Otitisexterna • Swimming • Frequent air travel
STAGES • Catarrhal stage • Stage of exudation • Stage of suppuration • Stage of healing • Stage of complication
Catarrhal stage • congestion of middle ear • Is characterized by occlusion of eustachian tube Stage of exudation • Exudates collect in the middle ear and ear drum • Ear drum is pushed laterally • Intiallyexudate is mucoid , later it becomes purulent
Stage of Suppuration • Pus in the middle ear • Increases pressure and stretches the ear drum • Perforates ear drum • Exudate start escaping into external auditory canal
Stage of healing • Treatment • Infection starts to resolve • Clears up completely without leaving any sequelae Stage of complication • left untreated • Infection spread to the mastoid antrum • Mastoiditis
PATHOPHYSIOLOGY Etiology Infection Eustachian tube Mediators of inflammation Chemotaxis of leucocytes
Increases vascular Permiability Middle ear inflammation Epithelial Secretory Activity (effusion) Sequale
CLINICAL MANIFESTATIONS Catarrhal Stage • Fullness or heaviness in the ear • Severe otalgia • Tinnitus • Autophony (spoken words of patient echo in the ears) • Cart wheel appearance of ear drum
Stage of exudation • Severe Catarrhal stage symptoms Stage of Suppuration • Perforation of the ear drum • Otorrhoea with mucoid purulent discharge • Pulsatile Discharge • Ear discharge with arterial dilation (Light house sign)
OTHER • Fever may rise to 104 to 106 F • Headache • Anorexia • Nausea • vomiting
DIAGNOSTIC EVALUATION • History collection • Physical examination • Otoscopy • Tympanocentesis • Culture and sensitivity of ear discharge • x-ray of the mastoid antrum
COMPLICATIONS • Peforation of ear drum • CSOM • Mastoiditis • Conductive hearing loss • Meningitis • Brain abscess
MANAGEMENT • To relieving the discomfort • To reduce the swelling • To eradicating the infection
Pharmacological treatment • Antibiotics • topical agents • Oral • Parenteral • Analgesics
Medications • Amoxicillin -80-90 mg / kg • Amoxicillin – 90mg/kg • Azithromycin – 30mg/kg (3 day course , ROM) • Clarithromycin – 15mg/kg • Clindamycin – 30-40 mg/kg IV • Ceftriaxone – 50 mg/ kg
Topical agents (ear drops) • For 10 days • 3-4 times a day • Ciprofloxacin / hydrocortisone (3 drops) • neomycin / hydrocortisone (4 drops) • Ofloxacin (5 drops)
Analgesics • Severe • Once daily • Actetaminophen – 15mg • Ibuprofen- 10mg • Diclo- 10mg Nasal decongestants Antihistamines
Glycerine cabolic ear drops/ Warm olive oil • Reduces pain • Before perforation
SURGICAL MANAGEMENT • Myringotomy • Myringoplasty
NURSING DIAGNOSIS • Acute pain related to inflammation and increased pressure in the middle ear as evidenced by pain scale score • Disturbed sensory perception , Auditory related to inflammation and edema in the middle ear as evidenced by hearing acuity test • Deficient knowledge regarding the disease condition and therapeutic regimen as evidenced by frequent doubts • Impaired verbal communication related to decreased hearing as evidenced by frequently asking to repeat.
ACUTE PAIN • Assess the characteristics of pain- severity, type • Advice the client to lie down in side lying position with affected ear downwards and raise head with pillow. • Hot water bag • Ice pack pack application • Analgesics • Antibiotics
DISTURBED SENSOR PERCEPTION , AUDITORY • Assess the clients hearing ability • Reduce unnecessary environmental noise • Encourage the family members to speak in a loud and clear voice • Notify the changes in hearing ability • Reassure the patient hearing loss is not permanent and will resolve with treatment. • Strict adherence to the antibiotic treatment
CONCLUSION • Otitis media is a group of inflammatory diseases of the middle ear. The two main types are acute otitis media and otitis media with effusion. AOM is an infection of abrupt onset that usually presents with ear pain. In young children this may result in pulling at the ear, increased crying, and poor sleep, decreased eating and a fever may also be present.
EVALUATION • What is ASOM. • What are the causes of ASOM. • Describe the stages of ASOM. • Eneumerate the pathophysiology of ASOM. • Enlist the clinical features of ASOM. • Explain the management of ASOM.
REFERENCE • Smeltzer – Brunner & Suddharth Textbook of Medical Surgical Nursing, Wolterskluwer publishers, 12th edition 2009. • Black – Medical Surgical Nursing, Elsevier publishers, 8th edition 2009. • Nettina – Lippincott manual of Nursing Practice, Wolterskluwer publishers, 7th edition 2014. • Lewis – Medical Surgical Nursing, Elsevier publishers, 10th edition, 2017