Download
1 / 42
430 likes | 698 Views
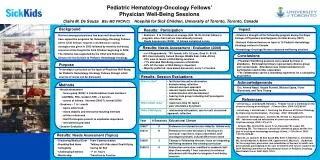
Pediatric Hematology Oncology Labwork Interpretation. Linda Ballard, CPNP, APRN. Heme/Onc Lab Interpretation. I’m freaking out- the platelet count is 20 k!!. Okay, so a low platelet count by itself isn’t always leukemia!. Components of the CBC. White blood cells (WBC) Red blood cells (RBC)

E N D
Pediatric Hematology Oncology Labwork Interpretation Linda Ballard, CPNP, APRN
Heme/Onc Lab Interpretation • I’m freaking out- the platelet count is 20 k!!
Okay, so a low platelet count by itself isn’t always leukemia!
Components of the CBC • White blood cells (WBC) • Red blood cells (RBC) • Platelets (PLT)
BONE MARROW PROGENITORS • Bone marrow precursors produce • WBC • RBC • Platelets
White Blood Cells • Normal lifespan is hours to days • Primary responsibility…..fight infection • Normal range~4-15,000 • Race variation • Age variation
White Blood Cells • Differential • Neutrophils • Lymphocytes • Monocytes • Eosinophils • Basophils
White Blood Cells • Neutrophils; also called Segs • Most numerous ~31-75% • Shortest lifespan • Band=immature form • “Left shift” • Myelocytes/Metamyelocytes
White Blood Cells--Neutrophils • Increased by • Infections, stress response, inflammatory disease, childbirth, ischemic necrosis • Decreased by • Infection, hypersplenism, SLE, chemotherapy, radiation therapy • Autoimmune process
White Blood Cells-Lymphocytes • Lymphocytes • Normal range 35-61% • Produced in lymph nodes and thymus • Increased by: infection, mononucleosis, thyrotoxicosis, ulcerative colitis, leukemia • Decreased by: steroids, immunosuppressants, renal failure
White Blood Cells-Monocytes • 2nd line of defense after neutrophils • Phagocytosis…..think Pac-man • Normal range 4-7% • Increased by: infection, leukemia, TB, RMSF, malaria, ulcerative colitis, mono • Decreased by: infection, bone marrow failure/leukemia
White Blood Cells--Eosinophils • Normal range 2-4% • Most commonly produced in response to • parasitic infections • allergic disorders • Other stimulants: leukemia, Hodgkin, ulcerative colitis, scarlet fever • Decreased production: stress, Cushings
White Blood Cells---Basophils • Normal range 0-1% • Increased by: chronic inflammation, hypersensitivity reactions • Decreased by: Steroids, hyperthyroidism
White Blood Cell--ANC • Absolute Neutrophil Count= ANC • ANC=WBC x (neutrophils/segs +bands) • Important predictor of immune function/reserve • Body’s ability to fight bacterial infections
Red Blood Cells • Normal lifespan is 120 days • Primary role is to carry hemoglobin • 2 primary regulatory factors • Tissue oxygenation • Renal production of erythropoietin
Red Blood Cells-Indices • Mean cellular volume(MCV) • Mean cellular hemoglobin(MCH) • Mean cellular hemoglobin concentration(MCHC) • Red cell distribution width(RDW)
Indices--MCV • Average size of the red cell • Normal range~75-94 • Morphology • Microcytic • Normocytic • Macrocytic
Microcytic RBC ( Low MCV) • Small size • Common causes: • Fe Deficiency • Lead poisoning • Thalassemia • Inflammation
Normocytic RBCs • Normal MCV=normal size • Normocytic anemia: • Early aplastic anemia • TEC • Leukemia/solid tumors • IBD/JRA • Sickle cell/hemolytic anemias • Renal disease
Macrocytic RBC’s (High MCV) • Large size=macrocytic • Common causes: • Nutritional • Liver disease, cyanotic heart disease • Hypothyroidism • Down’s Syndrome • Bone marrow failure
RBC indices--MCH • Mean cellular hemoglobin (MCH) • average weight of Hgb per RBC • generally rises and falls with MCV
Red Cell Indices-MCHC • Mean cellular hemoglobin concentration • measures the concentration of hemoblobin in the RBC • Hypochromic; pale appearing • Normochromic • Hyperchromic
Red Cell Distribution Width • RDW • Measures the uniformity of cell size • Range~11.5-14.5 • Increased in • Fe deficiency • B12/Folate deficiency • Sickle cell • Anisocytosis….variablity in the RBC size
Reticulocyte Count • Immature RBC • Measures hematopoesis from the bone marrow • 0.5-1.5% normal range
Reticulocytosis (High retic) • Indicates an overactive bone marrow • Hemolytic anemias • Sickle cell, AIHA, Hereditary spherocytosis • Acute blood loss
Reticulocytopenia (Low retic) • Indicates lack of RBC production in the bone marrow • Infection • Bone marrow failure syndromes • Folate/Fe deficiency/B12 anemias
Hemoglobin--Hgb • Part of RBC that binds oxygen and delivers to tissues in the body • Normal ranges based on age and gender • Physiologic nadir ~2mos. Of age
Hemoglobin--Hgb • Increased with: • Congenital heart disease • Chronic hypoxia • High altitudes • Polycythemia vera • Dehydration
Hemoglobin-Hgb • 3 major reasons for decreased hgb • Decreased production of RBC • Increased destruction of RBC • Blood loss
Hematocrit • Percentage of RBC to whole blood • In relation to Hemoglobin • usually 3 times the hemoglobin value • Affected by: • Dehydration • Stress • Vasocclusion
Platelets • Form a plug at the site of injury • Lifespan is 8-10 days • Normal range is 150-450k • 2/3 in circulating blood volume; 1/3 in spleen
Platelets • Thrombocytopenia • Decreased platelet count <150,000 • Causes: • Decreased production • Abnormal destruction • Abnormal pooling
Platelets • Thrombocytosis • Increased platelet count>600,000 • Causes: • Myeloproliferative disease • Acute blood loss • Polycythemia vera
Platelets--MPV • MPV=Mean platelet volume • Measures uniformity of platelet size • Increased: ITP, leukemia, splenectomy , vasculitis • Decreased: Wiskott Aldrich
Abnormal labs • Production vs Destruction • Quality vs Quantity • Acquired vs Congenital
Clinical Assessment • History • Activity level, appetite • Recent infections, fevers • Pain • Weight loss • Family medical hx
Clinical Assessment • Physical • Skin color • Bruising, bleeding • Rashes • Lymph nodes • Spleen, liver • Lung sounds
Other Labs • Chemistries • Bone Marrow • CSF
Case # 1 • Annie is a 2 year old referred for anemia. • Screening hgb at well check was 9.4. • Clinical sx to review? • Pt started on oral iron supplement 2 mg/kg/day • Recheck 2 mths later- CBC: WBC 6.8, Hgb 9.9, Hct 29, MCV 62, plt 224 k.
Case # 2 • Henry is 3 years old, brought to PCP for 4 days of worsening fever, lethargy, pallor. • Alert, VSS. • PE: enlarged spleen, scleral icterus, jaundice • CBC: WBC 9.4, Hgb 7.5, MCV 78, plt 257 k • retic 10.8
Case # 3 • Lucy is a 10 year old brought to PCP for a “rash” noted on chest, back and abdomen for a few days. • Other sx include fatigue, c/o leg pains. Low grade fever • CBC: WBC 35 K, Hgb 11, plt 34 K.
Summary • It’s not just about the numbers • History • Patient • Family • Physical findings • Full system exam • If the labs don’t match the clinical picture, repeat the lab!