Download
1 / 47
1.13k likes | 3.77k Views
Inflammatory disease of maxillofacial area ( odontogenic and non odontogenic ). Classification of inflammatory processes of MFA. Periostitis , osteomyelitis , abscess, plegmonas : etiology, pathogenesis, clinical course of, complications, prophylaxis.

E N D
Inflammatory disease of maxillofacial area (odontogenicand non odontogenic). Classification of inflammatory processes of MFA. Periostitis, osteomyelitis, abscess, plegmonas: etiology, pathogenesis, clinical course of, complications, prophylaxis. Course of maxillofacial surgery and stomatology of Tashkent Medical Academy, associate professor Sh.A.Boymuradov
Table of Content Overview General symptoms of inflammationClinical manifestations of inflammation Differential diagnosis Causes Spectrum of bacterial therapy Prevalence of different abscesses Classification of abscesses
Overview Inflammation is a defence reaction of the organism to local injuries of any type, to infection.Infection is a pathological state resulting from the invasion of the body by pathogenic microorganisms and their proliferation within the organism.
Inflammation diseases Non odontogenic Odontogenic
Non odontogenic inflammation diseases • 1. Fufuruncle • 2. Anthrex • 3. erysipelas • 4. Sibir canker • 5. Noma (gangrenuosstomstitis)
Non-odontogenic causes of soft tissue infections Infected fracture Infected soft tissue wounds or tumors Infection by foreign bodies Infection after injection Inflammatory of skin or mucosal membrane disorders Haematogeneous or lymphogeneious spreading
Complication of furuncle of the face: Tromboflibitis of vein
Odontogenic inflammation disesases of the face • 1. Acute odontogenicperiostitis • 2. Acute osteomyelitis of jaws • 3. Odontogenicabcsesses • 4. Odontogenicphlegmonas • 5. Odontogeniclymfadinitis
Classic signs of acute infection appear Heat Redness Tumor (oedema) Loss of function (trismus, difficult to swollow speech) Additional: leucocytosis and CRP increasis
CRP (C-reactive protein) is synthesised in the liver.It is one of the chemical mediators of inflammation and its serum level increases faster and to higher levels than that of any other parameters in acute infectious and non-infectious inflammation. Therefore, CRP belongs to the group of acute-phase proteins. These are blood lipids the concentration of which increases in the course of inflammatory diseases. CRP binds to invading foreign substances and activates important steps of the immune system with macrophages and the complement system. Due to its relatively short half-life of 24 hours, changes in CRP concentration indicate changes in the inflammatory process.
The clinical picture of acute periostitis of the jaws. • 1.Presence of causal teeth • 2. Smoothness of a transitive fold • 3. Fluctuation of a transitive fold • 4. Painful percussion of causal tooth • Increases of temperature up to 38 гр • Dysfunctions: opening of a mouth, chewing, speech, swallowing.
Tipes of osteomyelitis of the jaw on the pelationship of causes • 1. Odontogenigosteomylitis • 2. Traumatic osteomylitis • 3. Hematogenosteomylitits
The theory of progress of osteomylitis of jaws • 1. The infectious-embolic theory • Infringements innervationof jaws • The theory a sensitization
Stages of current of an osteomyelitis of jaws • 1. Acute • 2. under acute • 3. chronic
Clinical picture of a acute osteomyelitis • 1 Looseness of a causal tooth • Infringement of function: opening of a mouth, chewing, speeches and swallowing • Mobility of a several teeth • Smoothness of a transitive fold from two sides. • Rise in temperature of a body up to 41 гр. • Fever
Treatment of osteomyelitis of laws Elimination of cause (causal teeth extraction) Incision dischargeofpus Spreading of the abcsses cavity Osteoperforation of injure bone drainage of the pus cavity Facultativeantibiotictreatment
Types of abscesses and phlegmonas • 1. Superficial located • 2. middle deep located • 3. deep located
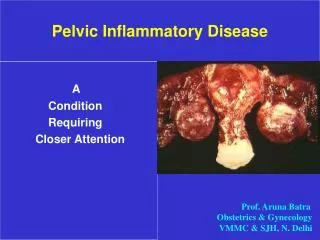
Abscess submucous abscess, smooth vestibuleLocalized collection of pus an a cavity caused by necrosis of tissue due to bacterial infection Demarcation by abscess mambrane (granulation tissue) Firm elastic consestence Fluctuation can be palpated only in superficial abscesses
Oedema Oedematous swelling of the ocular region in abscess of the canine fossa concomitant oedema of the upper lip in submucous abscess in region 11 accumulation of fluid in tissue classic sign of any acute inflammation (tumour)softandelasticonpalpation.Due to the anatomical situation in the maxillofacial region, the typical fluctuation of an abscess is absent in the majority of cases or only rarely identifiable
Differentialdiagnosis of abcsesses swelling caused by neoplasms (sarcomas, malignant lymphomas, carcinomas) salivaryglanddiseases
Phlegmon (cellulitis) diffusely spreading inflammation between superficial tissue levels (without being limited to them) No demarcation infection by highly virulent bacteria (release of lytic enzymes) impaired defence mechanisms of the organism serous-purulentandnecrotisinginflammation serous-purulentandnecrotisinginflammation firmtohard on palpation
Odontogenic causes of soft tissue infections In 92-94% of the cases, infections in the oro-maxillofacial region are of odontogenic origin Periapicalperiodontitis Infection after teeth extraction difficultdentition (pericoronitis) Marginal priodontitis infected retained root fragments
Anaerobic flora Odontogenic infections are always caused by a mixed flora of aerobic and anaerobic bacteria. The count of anaerobic bacteria always outnumbers that of aerobic bacteria (at least by 102). Pure anaerobic mixed infections also occur. Anaerobic bacteria play a predominant role in the generation and spreading of odontogenic soft tissue infections. Infection by clostridia as well as mixed infections by yeasts and bacteria may occur
Therapy The following statement that Galen made almost 2,000 years ago - "ubi pus, ibievacua" (if there is pus, remove it) which is still valid in the era of antibiotics could be considered the clinical conclusion from the abscess pathophysiology explained above. Therefore, incision and drainage are the primary therapy of an phlegmonas
Incision of an abscess is advisable, possibly by a sufficiently wide incision at the maximum point of the swelling. Obtain sufficient discharge of pus with the incision. Prepare for drainage of the purulent exudate In smaller abscesses, it is usually sufficient to insert a Iodoform gauze packing strip for 2-3 days; extensive abscess cavities are drained through a tube that is fixed in place with sutures
rinsing of the abscess Culture and antibiotic sensitivity testing Antibiotics for parenteral therapyInfections are classified as mild, moderate or severe infections.Differential surgical and antibiotic treatment is indicated according to the extension tendency and severity grade of infection as well as the general condition of the patient.